Fluid overload is often observed in patients with heart failure and secondary oliguric states. A thorough assessment of the fluid status of the patient may help guide the therapy and prevent complications induced by inappropriate therapeutic strategies.The present publication is divided into four parts: Definition and Classification, Pathophysiology, Diagnosis and Therapy. In the first section, the authors present new definitions for heart failure, acute kidney injury and cardiorenal syndromes to facilitate the process of understanding the complex link between the heart and the kidney. Subsequently, different conditions leading to fluid overload are described, followed by an account of emerging diagnostic tools, therapies and technologies devoted to the treatment of patients with severe fluid-related disorders. Clearly structured and written, the present book is a practical tool for physicians and professionals involved in the management and care of patients with combined heart and kidney disorders. Moreover, it also serves as a reference textbook for medical students, residents and fellows dealing in everyday practice with fluid overloaded and oliguric patients.
eBook - ePub
Fluid Overload
Diagnosis and Management
- 252 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Fluid Overload
Diagnosis and Management
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
CardiologyDiagnosis
Ronco C, Costanzo MR, Bellomo R, Maisel AS (eds): Fluid Overload: Diagnosis and Management.
Contrib Nephrol. Basel, Karger, 2010, vol 164, pp 88–117
Contrib Nephrol. Basel, Karger, 2010, vol 164, pp 88–117
______________________
Use of Biomarkers in Evaluation of Patients with Heart Failure
Leo Slavina · Lori B. Danielsa · Alan S. Maisela,b
aDivision of Cardiology, University of California, San Diego, Calif., bVeterans Affairs Medical Center, San Diego, Calif., USA
______________________
Abstract
Despite advances in the understanding of the pathophysiology of heart failure, its diagnosis and management still remain challenging. Biomarkers have added significant value to the clinical evaluation of heart failure. While their use is not intended as a substitute for clinical judgment, their relevance in diagnosis, management, and prognosis has been proven. This review focuses on biomarkers resulting from hemodynamic stress, injury and inflammation, and their clinical relevance in modern practice.
Copyright © 2010 S. Karger AG, Basel
Heart failure (HF) is a serious public health matter in modern medicine. HF, at its simplest conceptualization, is the inability to adequately propel blood forward leading to a devastating cascade of events resulting in significant morbidity and mortality. The approach to the diagnosis of acute HF is complex and challenging due to its heterogeneous presentations and nonspecific signs and symptoms [1]. Classically, one is taught that a careful history in patients presenting with congestive HF (CHF) will elicit symptoms of dyspnea, orthopnea, and paroxysmal nocturnal dyspnea, while the physical exam will reveal elevated jugular venous pressure, rales, an S3 gallop, and pitting peripheral edema. However, it is well documented that, in practice, the clinical presentation of HF, even in combination with chest X-rays, electrocardiograms, and standard laboratory assessments, frequently does not clinch the diagnosis. Oftentimes, the clinician must entertain other etiologies of dyspnea such as chronic obstructive pulmonary disease or pneumonia, which can delay necessary treatment. The emergence of various classes of biomarkers is leading to a better understanding of the pathogenesis, diagnosis, and prognosis in HF.
Table 1. Desired properties of an ideal biomarker
Health-care-related features | Test-related features |
Give objectivity to evaluation and diagnosis of patients, especially those in whom signs and symptoms are not very sensitive or specific | High sensitivity and specificity |
Help with correct triage by assessment of prognosis and risk stratification | Reproducibility and accuracy |
Help to objectively guide the therapy or management | Low coefficient of variation |
Enable an optimum screening process | Easy to perform and analyze, possibly a point of care test |
Guide the delivery of cost-effective medical care | Applicable across sexes, ethnicity and age spectra |
Make physiological sense | |
Adapted from Maisel etal. [2]. |
Biomarkers in Heart Failure
Introduction
Table 1 demonstrates the desired properties of an ideal biomarker [2]. The biomarker should be highly reproducible, readily available, cost-effective, and have added value in the clinical decision-making process. There are currently few biomarkers that can fulfill all of these requirements. Biomarkers that do meet these criteria reflect a number of different mechanisms such as biomechanical stretch, inflammation and myocyte injury that are involved in the pathophysiology of HF. These markers individually and jointly provide important information in assessing the progression of disease, diagnosing acute exacerbations, and providing prognostic information.
Markers of Myocardial Stretch
Natriuretic Peptides
Biology
There are three major natriuretic peptides (NPs), atrial NP (ANP), B-type NP (BNP), and C-type NP (CNP), all of which counter the effects of volume overload or adrenergic activation of the cardiovascular system (table 2). ANP is primarily synthesized in the atria, stored in granules, and under minor triggers such as exercise is released into the circulation [3]. BNP has minimal storage in granules and is synthesized and secreted in bursts primarily by the ventricles [3]. CNP is a product of endothelial cells and may be protective in postmyocardial infarction remodeling [4]. Upon release into the circulation, ANP and BNP bind to various tissues and induce vasodilation, natriuresis, and diuresis [5].
Table 2. NP subtypes and their actions
NP | Actions |
ANP | arterial vasodilation, venodilation, natriuresis, diuresis, antagonizes reninaldosterone-angiotensin system, increases renal GFR |
BNP | arterial vasodilation, venodilation, natriuresis, diuresis, antagonizes reninaldosterone-angiotensin system, antiproliferative |
CNP | arterial vasodilation, venodilation, natriuresis, diuresis, antagonizes reninaldosterone-angiotensin system, antiproliferative |
Left ventricular pressure or volume overload results in myocardial wall stress that initiates the synthesis of pre-proBNP. Pre-proBNP is initially cleaved to proBNP and then to BNP, the biologically active form, and the inactive N-terminal fragment, NT-pro BNP (fig. 1). The mechanism of action of NPs is mediated through membrane-bound NP receptors (NPRs). NPR-A preferentially binds ANP and BNP, and NPR-B primarily binds CNP. The NP-receptor interaction activates the enzyme guanylyl cyclase, leading to the production of cyclic guanosine monophosphate. Clearance of NPs is mediated through NPR-C, degradation by neutral endopeptidase, and direct renal clearance.
Patients with HF are in a state of BNP insufficiency resulting from a deficiency of the active BNP form plus molecular resistance to its effects [6]. Studies have demonstrated that the BNP detected in acute HF is primarily the high-molecular-weight proBNP rather than the biologically active form [7]. Some have suggested that abnormal cellular processing of BNP is a factor in the relative BNP deficiency state in HF [8]. Additionally, upregulation of phosphodi-esterases leads to rapid clearance of the secondary messenger, cyclic guanosine monophosphate, despite high activation of the NPRs by NPs [9].
What constitutes a normal NP level depends on the specific clinical setting. Two studies found that BNP levels in normal adults without cardiovascular disease increase with age and appear to be higher in women, with NT-pro BNP levels showing greater age dependence than BNP levels [10, 11]. General guidelines are that in young, healthy adults, 90% will have BNP <25 pg/ml and NT-proBNP ≤ 70 pg/ml [12]. In patients presenting with acute dyspnea, cutoffs of BNP <100 pg/ml, and NT-proBNP <300 pg/ml should be used to exclude HF [13, 14].
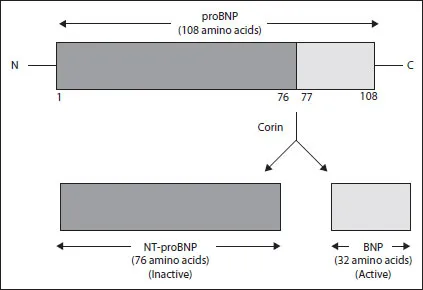
Fig. 1. Synthesis and processing of BNP.
Natriuretic Peptides in Acute Heart Failure
BNP and NT-proBNP have become powerful diagnostic tools in the evaluation of patients presenting with dyspnea in a variety of clinical settings. In the Breathing Not Properly Multinational Study, BNP levels were measured in 1,586 patients with shortness of breath upon arrival in the Emergency Department (ED). Use of BNP resulted in a higher diagnostic accuracy, with an area under the receiver-operating characteristic curve (AUC) of 0.91 [13]. A BNP cut-point of 100 pg/ml was 90% sensitive and 76% specific for the diagnosis of HF as the cause of dyspnea (fig. 2). The data were extended to NT-proBNP in the PRIDE (ProBNP Investigation of Dyspnea in the ED) study, which measured NT-proBNP in 600 ED patients with dyspnea and demonstrated its sensitivity and specificity in the diagnosis of CHF (AUC = 0.94) [14]. The cut-point of NT-proBNP <300 pg/ml was proposed to rule out HF as the etiology.
...Table of contents
- Cover Page
- Front Matter
- Heart Failure: Pathophysiology and Clinical Picture
- Heart Failure Classifications – Guidelines
- Acute Kidney Injury: Classification and Staging
- Cardiorenal Syndromes: Definition and Classification
- Oliguria and Fluid Overload
- Pathophysiology of Fluid Retention in Heart Failure
- Fluid Overload as a Biomarker of Heart Failure and Acute Kidney Injury
- Fluid Balance Issues in the Critically Ill Patient
- Prerenal Azotemia in Congestive Heart Failure
- Use of Biomarkers in Evaluation of Patients with Heart Failure
- Oliguria, Creatinine and Other Biomarkers of Acute Kidney Injury
- Current Techniques of Fluid Status Assessment
- Bioelectric Impedance Measurement for Fluid Status Assessment
- Diuretic Therapy in Fluid-Overloaded and Heart Failure Patients
- Pharmacological Therapy of Cardiorenal Syndromes and Heart Failure
- Extracorporeal Fluid Removal in Heart Failure Patients
- Technical Aspects of Extracorporeal Ultrafiltration: Mechanisms, Monitoring and Dedicated Technology
- Use of Brain Natriuretic Peptide and Bioimpedance to Guide Therapy in Heart Failure Patients
- Fluid Management in Pediatric Intensive Care
- Fluid Assessment and Management in the Emergency Department
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Fluid Overload by C. Ronco,M. R. Costanzo,R. Bellomo,A. S. Maisel, Claudio Ronco in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.