eBook - ePub
Health and Nutrition in Adolescents and Young Women: Preparing for the Next Generation
80th Nestlé Nutrition Institute Workshop, Bali, November 2013
- 144 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Health and Nutrition in Adolescents and Young Women: Preparing for the Next Generation
80th Nestlé Nutrition Institute Workshop, Bali, November 2013
About this book
Nutrition of young women and its effect on offspring is an almost neglected topic in developed and developing countries alike. Under- as well as overnutrition of the mother can negatively program the child's health: Maternal undernutrition and micronutrient deficiencies are related to both low birth weight and intrauterine growth retardation. Moreover, they also result in negative epigenetic programming both during conception and in the newborn. Obese mothers, on the other hand, may produce offspring with a lower life expectancy, a fact which could be related to the higher risk of developing metabolic syndrome in adult life. This book provides insights into the influence of maternal health and nutrition on both fetal and postnatal growth and health of the offspring. Contributions focus on future mothers from their adolescence to pregnancy, thus providing valuable information for the clinician involved in the care of adolescents and young women.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaSubtopic
Nutrición, dietética y bariatríaGlobal Epidemiology and Risk Factors
Bhutta ZA, Makrides M, Prentice AM (eds): Health and Nutrition in Adolescents and Young Women:
Preparing for the Next Generation. Nestlé Nutr Inst Workshop Ser, vol 80, pp 1-14,
(DOI: 10.1159/000360147) Nestec Ltd., Vevey/S. Karger AG., Basel, © 2015
Preparing for the Next Generation. Nestlé Nutr Inst Workshop Ser, vol 80, pp 1-14,
(DOI: 10.1159/000360147) Nestec Ltd., Vevey/S. Karger AG., Basel, © 2015
______________________
Adolescent Health Globally: Issues and Challenges
George C. Patton · Susan M. Sawyer
Centre for Adolescent Health, University of Melbourne, Melbourne, VIC, Australia
______________________
Abstract
Rapid declines in fertility, increasing survival through infancy and childhood and greater longevity mean that this generation of adolescents will be the largest in human history. In low-income countries, the ‘youth bulge’ has the potential to bring great economic prosperity. In contrast, many high-income countries face a ‘demographic cliff’ where a smaller pool of young people poses major economic and social challenges. In both contexts, the health and well-being of this generation of adolescents will determine future national development. Shifts in adolescent development have major implications for health. Falls in the age of puberty together with a rising age of marriage have, for example, given rise to more sexually active unmarried adolescents. In settings where healthcare needs are well met, the benefits are clear in terms of lower pregnancy rates, lower maternal mortality and lower rates of HIV and other sexually transmitted diseases. Conversely, where this shift occurs in settings with poor adolescent health care, where sexual activity in young unmarried women is stigmatized and where poverty forces young women into early marriage or selling sex, both health and life outcomes can be catastrophic. In this context, poor and socially marginalized adolescents, particularly those out of school, without stable accommodation or family, or in juvenile detention, have the worst health profiles. The opportunities for gain or loss are great across all aspects of health in adolescence. It is during these years that the risks for injury and mental disorders are highest, and when risks for later-life noncommunicable diseases (cancer, cardiovascular and respiratory disease) such as tobacco use, obesity and inactivity are established. The great majority of adult mental disorders begin in adolescents. So too, injuries rise sharply with high rates of suicide, motor vehicle injury and violence, including sexual violence in these years. All will affect the future health, social adjustment and economic prospects of today's adolescents. It will in turn affect their capacities as parents and a healthy start to life for their children. There is great variation between countries, even within the same region, in patterns of adolescent health. For low-income countries, key indicators at national and district levels should include rates of maternal mortality, HIV and sexually transmitted diseases, age of onset of sexual activity, early childbirth, availability of contraception and age of marriage. Countries should also have data on adolescent nutrition including anemia, patterns of injury including sexual violence and coercion, mental health and disorder, and substance abuse. At a local level, data on family functioning (e.g. violence, conflict), educational engagement, peer behavior and community attitudes (e.g. to providing contraception to sexually active unmarried adolescents) are also needed to effectively guide programming and health service delivery. The evidence base for prevention in adolescence is stronger than ever before. Public health approaches that use multiple coordinated actions at national and local levels show great promise. These typically involve steps of using ‘best available’ data to evaluate local needs, identifying priority targets for intervention, implementing evidence-based programs and policies followed by monitoring, commonly using the same indicators that framed need.
© 2015 Nestec Ltd., Vevey/S. Karger AG, Basel
Adolescent Health and Development: A Global Perspective
Today's generation of adolescents is the largest in human history. 1.2 billion 10-to 19-year-olds comprise around 18% of the global population. Nearly 90% live in low- and middle-income countries (LMICs) where the ‘youth bulge’ may make up over a third of the country's population. In contrast, in most high-income countries (HICs), the proportion of young people in the population is at a historic low and represents a ‘youth deficit’.
Adolescence is commonly considered to begin with the completion of puberty and end with the transitions into marriage and parenthood. Although most societies have a similar concept of adolescence, there is little consistency in age definitions between countries. The term ‘young people’ commonly refers to the age group of 10 through to 24 years and is often the focus of policy attention. It is the focus for the current paper, with three distinct age brackets of 10-14 years (early adolescence), 15-19 years (late adolescence) and 20-24 years (young adulthood).
Downward trends in the age of puberty (and thus adolescence) commenced in the 19th century for today's HICs almost certainly following better childhood nutrition (fig. 1a). This trend attenuated by the 1960s when the mean age of menarche in girls stabilized between 12 and 13 years [1] (fig.1b). There have been similar more recent downward trends in the age of menarche in LMICs [1]. In low-income settings, there is a strong correlation between age of menarche, age of first marriage and birth of first child, a relationship that can be changed by staying in school [2]. Puberty is accompanied by changes in brain function, particularly in the limbic system and subcortical structures involved in emotional processing. One result is a greater intensity of emotional experiences and a life phase in which health problems related to emotion and emotional control (e.g. injury, violence and mental health) are common [3].
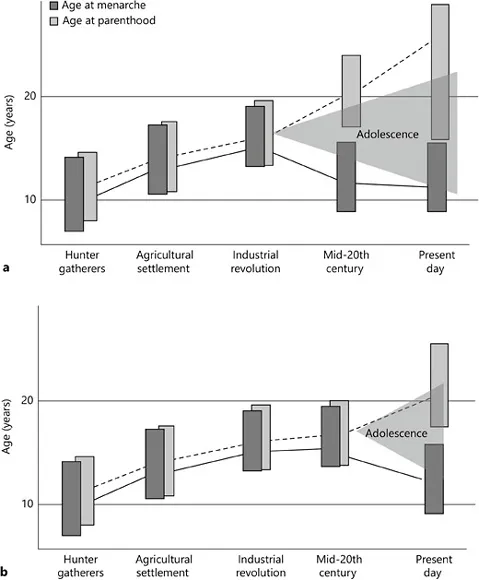
Fig. 1. a Changing shape of adolescent development in today's HICs. b Changing shape of adolescent development in today's LMICs. Adapted from Gluckman and Hanson [32].
There have also been a striking upward extensions in the age at which adult social roles and responsibilities are adopted. In preindustrial societies, the gap between physical maturation and parenthood was generally around 2 years for girls and 4 years for boys [4]. In many HICs, first marriage and parenthood now commonly occur 15-20 years after the onset of puberty. Inter-related drivers of this upward extension include industrialization, length of education and urbanization. Transitions into marriage and childrearing commonly brought a ‘maturing out’ of risky adolescent behaviors, including tobacco, alcohol and illicit substance use. With a longer adolescence, young people often come to parenthood with more established and dependent patterns of alcohol and other substance use that may no longer be as readily reduced. So too, obesity is more prevalent in both middle- and high-income countries with heightened risks for infertility and pregnancy complications such as gestational diabetes and hypertension [5].
Longer duration of adolescence is evident in all but the poorest of countries [6]. In LMICs, there are commonly differences in both pubertal timing and transitions into marriage and parenthood between wealthier urban and poorer rural settings. With economic development, traditional linear sequences of social role transitions, e.g. finishing school, getting a job, getting married and having children, are generally less well defined. In settings with good health care, the delays in transition to marriage and parenthood have led to extraordinary reductions in maternal mortality and morbidity.
The pubertal maturation of the limbic system stands in contrast to the later maturation of the brain regions involved in emotional control. Maturation of the prefrontal cortex (PFC) involved in planning, inhibiting inappropriate responses and decision-making continues across adolescence until at least the third decade. The greatest disparity in maturation of these systems (limbic vs. PFC) is during early to mid-adolescence. This developmental imbalance in emotional control favors behaviors driven by emotion and rewards over rational decision-making. Adolescents engage in risky behaviors despite knowledge of risks particularly in the presence of peers [7]. This is also relevant when considering the media that can act as a ‘super-peer’. Indeed, the media's contribution to adolescent sexual health risks in East Asia has been shown to be equivalent to the influence of peers, families or schools [8]. The wider implications of brain maturation on policies and programming are only starting to be explored. However, current understandings suggest the value of social structures to support the emerging capacity of adolescents in decision making. Such structures are likely to have elements that promote ‘connectedness’ and others that promote ‘regulation’ or setting clear rules and values [9]. These understandings reinforce the value of strategies that promote a graded exposure to health risks, such as graduated driving licenses.
Adolescent Health Risks and Problems
The chapter draws on the conceptual framework used in the recent Lancet series to describe adolescent health and its determinants within the life course [10] (fig. 2).
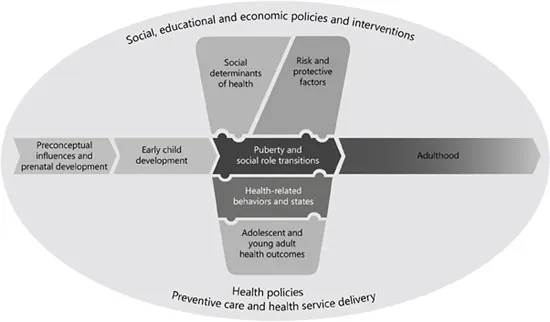
Fig. 2. A conceptual framework for adolescent health.
There are profound reciprocal relationships between adolescent h...
Table of contents
- Cover Page
- Front Matter
- Global Epidemiology and Risk Factors
- Role of Nutrition in Adolescent Health
- Interventions
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Health and Nutrition in Adolescents and Young Women: Preparing for the Next Generation by Z. A. Bhutta,M. Makrides,A. M. Prentice,Z.A., Bhutta,M., Makrides,A.M., Prentice, Z. A. Bhutta, M. Makrides, A. M. Prentice in PDF and/or ePUB format, as well as other popular books in Medicina & Nutrición, dietética y bariatría. We have over 1.5 million books available in our catalogue for you to explore.