- 148 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Ultrasound imaging techniques are an indispensable complement to physical examination, which is often frustrating, if not useless, for diagnosing kidney problems. The application of ultrasound techniques in clinical routine helps clinicians to rule out, at first glance, some serious pathological conditions and to concentrate on the accurate diagnosis of the patient. Moreover, sonography can extend the spectrum of diagnostic criteria in acute kidney diseases. It makes it possible to determine morphological parameters without potentially toxic contrast media while exploring functional aspects with contrast enhanced or Doppler ultrasound techniques. This publication meets a growing demand for current information among physicians and nurses in the field. With a focus on the daily practice of diagnosing kidney disease, it is an important resource for both beginner and advanced users of ultrasound imaging techniques.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Medical Technology & SuppliesChronic Kidney Disease
Meola M, Petrucci I, Ronco C (eds): Ultrasound Imaging in Acute and Chronic Kidney Disease.
Contrib Nephrol. Basel, Karger, 2016, vol 188, pp 69-80 (DOI: 10.1159/000445469)
Contrib Nephrol. Basel, Karger, 2016, vol 188, pp 69-80 (DOI: 10.1159/000445469)
______________________
Imaging in Chronic Kidney Disease
Mario Meolaa, b · Sara Samonia, c · Ilaria Petruccia, b
aSant'Anna School of Advanced Studies, Pisa, bDepartment of Internal Medicine, University of Pisa, Pisa, and cDepartment of Nephrology Dialysis and Transplantation, International Renal Research Institute (IRRIV), San Bortolo Hospital, Vicenza, Italy
______________________
Abstract
Chronic kidney disease (CKD) diagnosis and staging are based on estimated or calculated glomerular filtration rate (GFR), urinalysis and kidney structure at renal imaging techniques. Ultrasound (US) has a key role in evaluating both morphological changes (by means of B-Mode) and patterns of vascularization (by means of color-Doppler and contrast-enhanced US), thus contributing to CKD diagnosis and to the follow-up of its progression. In CKD, conventional US allows measuring longitudinal diameter and cortical thickness and evaluating renal echogenicity and urinary tract status. Maximum renal length is usually considered a morphological marker of CKD, as it decreases contemporarily to GFR, and should be systematically recorded in US reports. More recently, it has been found to be a significant correlation of both renal longitudinal diameter and cortical thickness with renal function. Conventional US should be integrated by color Doppler, which shows parenchymal perfusion and patency of veins and arteries, and by spectral Doppler, which is crucial for the diagnosis of renal artery stenosis and provides important information about intrarenal microcirculation. Different values of renal resistive indexes (RIs) have been associated with different primary diseases, as they reflect vascular compliance. Since RIs significantly correlate with renal function, they have been proposed to be independent risk factors for CKD progression, besides proteinuria, low GFR and arterial hypertension. Despite several new applications, US and color Doppler contribute to a definite diagnosis in <50% of cases of CKD, because of the lack of specific US patterns, especially in cases of advanced CKD. However, US is useful to evaluate CKD progression and to screen patients at risk for CKD. The indications and the recommended frequency of color Doppler US could differ in each case and the follow-up should be tailored.
© 2016 S. Karger AG, Basel
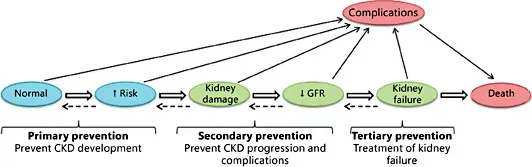
Fig. 1. Conceptual model of CKD. Algorithm represents the CKD progression, from the development to the occurrence of complications. Green circles symbolize CKD stage 3-5, blue circles preclinical phases (CKD stages 1-2 and increased risk for CKD), while pink circles the major outcomes such as end-stage renal disease and death. Thin arrows indicate risk factors related to the development and the progression of CKD. Empty arrows symbolize the potential reversibility of clinical phases. Complications represent the clinical manifestations due to CKD and its treatment as well as the consequences of the reduction of GFR and cardiovascular diseases associated to CKD. The objectives of primary, secondary and tertiary CKD prevention are to slow CKD progression, treat complications of CKD and reduce cardiovascular risk, thus improving patients’ life quality and survival. Modified from National Kidney Foundation guidelines [2].
Definition, Staging and Progression of Chronic Kidney Disease
The National Kidney Foundation's Kidney Disease Quality Outcome Initiative (NKF-KDOQI) [1] has proposed the current conceptual model of chronic kidney disease (CKD) for the first time in 2002. Subsequently, this model was improved by the Kidney Disease: Improving Global Outcomes work group and, at last, approved in an international consensus conference in 2005 [2]. The conceptual model of CKD, showed in figure 1, contributed to improve definition, staging, prognosis, treatment and complications of CKD, as well as risk factors for CKD progression. The objective of this model was to develop programs for primary CKD prevention and improve outcomes in advanced stages of CKD (secondary and tertiary CKD prevention). Despite current clinical management of nephropathic patients including several strategies to slow CKD progression, reduce cardiovascular risk and treat CKD complications, thus improving patients’ life quality and survival, there are still unsolved problems, such as the assessment of the impact of CKD on cardiovascular risk, the high frequency of late referral of nephropathic patients to nephrologists, the evaluation of the precise relationship between acute kidney injury (AKI) and CKD and the potential reversibility of CKD. Moreover, the definition of a normal range of values for glomerular filtration rate (GFR) in the elderly is still controversial, as well as the clinical meaning of albuminuria in CKD patients. A multidisciplinary approach, including the analysis of epidemiological data, basic research and clinical investigations, may assess the efficacy of each therapeutic strategy and its ability to decrease the social burden of CKD.
Table 1. Stages of CKD
Stage | Description | GFR, ml/min/1.73 m2 |
1 | Kidney damage with normal or ↑ GFR | ≥90 |
2 | Kidney damage with mild ↓ GFR | 60-89 |
3 | Moderate ↓ GFR | 30-59 |
4 | Severe ↓ GFR | 15-29 |
5 | Kidney failure | <15 (or dialysis) |
CKD is defined as either kidney damage or GFR <60 ml/min/1.73 m2 for ≥3 months. Kidney damage is defined as pathologic abnormalities or markers of damage, including abnormalities in blood or urine tests or imaging studies. | ||
CKD is diagnosed by the presence of either kidney damage or decreased kidney function (decreased GFR) for ≥3 months [1-3]. This definition provides objective diagnostic criteria, which can be easily checked by means of blood or urine samples or renal imaging.
The Cockcroft-Gault and the Modified Diet in Renal Disease equations are the most used formulas to estimate, respectively, creatinine clearance (CrCl) and GFR. They are both precise if GFR is less than 60 ml/min/1.73 m2, while they lose accuracy in the presence of higher GRF values. In clinical settings where renal function must be precisely assessed, such as in potential kidney donors, 24-hour CrCl measurement is mandatory. However, in most cases, estimated GFR (eGFR) allows diagnosis, classification and evaluation of CKD progression [1, 3]. The CKD classification in 5 stages, based on the progressively worsening of GFR, is shown in table 1.
The aims of each therapeutic strategy used in CKD are to prevent the loss of renal function, to manage potential complications and to reduce cardiovascular risk.
The loss of renal function in CKD may widely vary. The rapid progression of CKD is defined as the decrease of GFR >4 ml/min/1.73 m2/year. When it occurs, CKD stage 3 (GFR <60 ml/min/1.73 m2) takes about 10 years to evolve in CKD stage 5 (15 ml/min/1.73 m2). The progression of CKD occurs more rapidly in patients suffering from poorly controlled arterial hypertension, proteinuria and diabetes [4], while it slows by the administration of renin-angiotensin system inhibitors, which reduces both blood pressure and proteinuria.
The most common complications of CKD are arterial hypertension, anemia, malnutrition, mineral bone diseases, neuropathy and worsening of life quality. These complications mainly occur during CKD stage 4 and 5 (GFR <30 ml/min/1.73 m2), but they may be prevented by early treatments. Moreover, it must be highlighted that CKD patients have a higher susceptibility to AKI related to surgical or medical potentially invasive procedures or exposure to toxic drugs than general population.
The presence of CKD is an independent risk factor for cardiovascular disease [5]. In CKD patients, cardiovascular events occur more frequently; treatment and prevention of cardiovascular diseases may both improve primary outcomes and reduce CKD progression, thus revealing a close linkage between heart and kidney [5, 6].
Prevalence and Etiology of CKD
CKD is a major cost driver for healthcare systems in developed countries. In fact, the number of patients with CKD is increasing due to the rise in the average population age and, subsequently, in the prevalence of age-related diseases, such as arterial hypertension and diabetes, that participate to the pathogenesis of CKD. Otherwise, CKD patients have 3- to 4-fold increased risk for cardiovascular mortality and 20- to 50-fold increased risk for dialysis, which is an expensive chronic treatment, compared to general population. It has been calculated that 363 patients per million population (pmp) started dialysis in 2013 in the United States [7].
Table 2 s...
Table of contents
- Cover Page
- Front Matter
- Acute Kidney Disease
- Chronic Kidney Disease
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Ultrasound Imaging in Acute and Chronic Kidney Disease by M. Meola,I. Petrucci,C. Ronco,M., Meola,I., Petrucci,C., Ronco, Claudio Ronco,Claudio, Ronco in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Technology & Supplies. We have over 1.5 million books available in our catalogue for you to explore.