![]()
PART ONE
Conceptual Foundations of Public Health Law and Ethics
![]()
CHAPTER ONE
Law and the Public’s Health
Mapping the Terrain
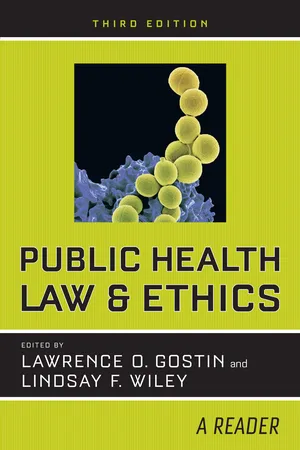
PHOTO 1.1. A doctor gives a typhoid inoculation at a rural school in Texas, 1943. Typhoid fever, a bacterial infection with a high fatality rate, was once common in the United States. Incidence decreased rapidly in the 1940s due to improvements in sanitation (especially chlorination of drinking water), development of effective antibiotic treatments, and vaccination. Today, there are only about 400 cases of typhoid in the United States each year, the vast majority among travelers returning from regions where infection remains endemic. Routine vaccination of schoolchildren is no longer recommended, but voluntary vaccination of travelers is crucial to protect the public’s health, particularly in light of the growing prevalence of multidrug-resistant strains of typhoid. Photograph by John Vachon for the Farm Security Administration.
The theory and practice of public health raise questions that are not resolved solely through scientific inquiry; rather, law and ethics guide the public health enterprise alongside epidemiology and biostatistics. Despite the close interplay among public health science, law, and ethics, each has its own methods and terminology. Until recently, cross-fertilization was rare. Most scholars and practitioners in the fields of law and ethics who have engaged in sustained examination of issues in health have focused principally on the financing and delivery of medical care and the conduct of medical research. The distinct perspectives and practices of public health have received far less attention. Fortunately, a growing number of practitioners, scholars, and organizations are developing public health law and public health ethics into fully fledged fields that stand alongside the related fields of health care law and bioethics.
Before applying ethics or law to problems in public health, it is important first to understand what we mean by public health. In this chapter, we highlight the prevention orientation, population perspective, and commitment to social justice that distinguish public health from medicine. We describe evolving models of public health science and practice, culminating in the social-ecological model. We conclude by surveying an ongoing debate over the legitimate scope of public health law, triggered by increased attention to noncommunicable diseases (e.g., cancer, heart disease, diabetes), injuries (e.g., motor vehicle, firearm, and overdose fatalities), and the social, economic, and environmental determinants of health in recent decades.
THE PREVENTION ORIENTATION AND THE POPULATION PERSPECTIVE
Public health inquiries and interventions are aimed at the prevention of injury, disease, and premature death at the population level. The Institute of Medicine (IOM) (1988, 19) in its landmark report The Future of Public Health proposed one of the most influential contemporary definitions of public health: “Public health is what we, as a society, do collectively to assure the conditions for people to be healthy.” The IOM’s emphasis on cooperative and mutually shared obligation (“we, as a society”) reinforces that collective entities (e.g., governments and communities) take responsibility for healthy populations. The definition also adopts a broad focus on social, environmental, cultural, and economic factors (“the conditions for people to be healthy”) that shape health-related behaviors and outcomes.
In the excerpt that follows, Rose offers a comparison between how medicine and public health approach questions of causation and methods for prevention. “Why did this patient get this disease at this time?” is a common question in medicine, underscoring a physician’s principle concern for individuals. By contrast, those interested in public health seek knowledge about why ill health occurs in the population and how it can be prevented through structural, rather than individual, interventions.
SICK INDIVIDUALS AND SICK POPULATIONS1
Geoffrey Rose
THE DETERMINANTS OF INDIVIDUAL CASES
In teaching epidemiology to medical students, I have often encouraged them to consider a question which I first heard enunciated by Roy Acheson: “Why did this patient get this disease at this time?” It is an excellent starting point, because students and doctors feel a natural concern for the problems of the individual. Indeed, the central ethos of medicine is seen as an acceptance of responsibility for sick individuals.
It is an integral part of good doctoring to ask not only, “What is the diagnosis, and what is the treatment?” but also, “Why did this happen, and could it have been prevented?” Such thinking shapes the approach to nearly all clinical and laboratory research into the causes and mechanisms of illness. Hypertension research, for example, is almost wholly preoccupied with the characteristics which distinguish individuals at the hypertensive and normotensive ends of the blood pressure distribution. Research into diabetes looks for genetic, nutritional and metabolic reasons to explain why some people get diabetes and others do not. The constant aim in such work is to answer Acheson’s question, “Why did this patient get this disease at this time?”
The same concern has continued to shape the thinking of all of us who came to epidemiology from a background in clinical practice. The whole basis of the case-control method [(a retrospective study design in which researchers compare the history of individuals who have a condition [“cases”] to the history of individuals who do not [“controls”])] is to discover how sick and healthy individuals differ. Equally the basis of many cohort studies [(prospective studies in which researchers follow a group of similarly situated individuals over time to see which of them develops the condition of interest)] is the search for “risk factors,” which identify certain individuals as being more susceptible to disease; and from this we proceed to test whether these risk factors are also causes, capable of explaining why some individuals get sick while others remain healthy, and applicable as a guide to prevention. . . .
Unfortunately this approach to the search for causes, and the measuring of their potency, has to assume a heterogeneity of exposure within the study population. If everyone smoked 20 cigarettes a day, then clinical, case-control and cohort studies alike would lead us to conclude that lung cancer was a genetic disease; and in one sense that would be true, since if everyone is exposed to the necessary agent, then the distribution of cases is wholly determined by individual susceptibility. Within Scotland and other mountainous parts there is no discernible relation between local cardiovascular death rates and the softness of the public water supply. The reason is apparent if one extends the enquiry to the whole of the UK. In Scotland, everyone’s water is soft [meaning that it contains low levels of calcium and magnesium]; and the possibly adverse effect becomes recognizable only when study is extended to other regions which have a much wider range of exposure. . . . Even more clearly, a case-control study of this question within Scotland would have been futile. Everyone is exposed, and other factors operate to determine the varying risk. Epidemiology is often defined in terms of study of the determinants of the distribution of the disease; but we should not forget that the more widespread is a particular cause, the less it explains the distribution of cases. The hardest cause to identify is the one that is universally present, for then it has no influence on the distribution of disease.
THE DETERMINANTS OF POPULATION INCIDENCE RATE
I find it increasingly helpful to distinguish two kinds of etiological question. The first seeks the causes of cases, and the second seeks the causes of incidence. “Why do some individuals have hypertension?” is a quite different question from “Why do some populations have much hypertension, whilst in others it is rare?” The questions require different kinds of study, and they have different answers. . . .
To find the determinants of prevalence and incidence rates, we need to study characteristics of populations, not characteristics of individuals. . . . Within populations it has proved almost impossible to demonstrate any relation between an individual’s diet and his serum cholesterol level; and the same applies to the relation of individual diet to blood pressure and to overweight. But at the level of populations it is a different story: it has proved easy to show strong associations between population mean values for saturated fat intake versus serum cholesterol level and coronary heart disease incidence, sodium intake versus blood pressure, or energy intake versus overweight. The determinants of incidence are not necessarily the same as the causes of cases. . . .
PREVENTION
These two approaches to etiology—the individual and the population-based—have their counterparts in prevention. In the first, preventive strategy seeks to identify high-risk susceptible individuals and to offer them some individual protection. In contrast, the “population strategy” seeks to control the determinants of incidence in the population as a whole.
The “High-Risk” Strategy
This is the traditional and natural medical approach to prevention. If a doctor accepts that he is responsible for an individual who is sick today, then it is a short step to accept responsibility also for the individual who may well be sick tomorrow. Thus screening is used to detect certain individuals who hitherto thought they were well but who must now understand that they are in effect patients. . . .
What the “high-risk” strategy seeks to achieve is something like a truncation of the risk distribution. This general concept applies to all special preventive action in high-risk individuals—in at-risk pregnancies, in small babies, or in any other particularly susceptible group. It is a strategy with some clear and important advantages. . . .
The “high-risk” approach offers a more cost-effective use of limited resources. . . . [I]t is more effective to concentrate limited medical services and time where the need—and therefore also the benefit—is likely to be greatest. . . . If intervention must carry some adverse effects or costs, and if the risk and cost are much the same for everybody, then the ratio of the costs to the benefits will be more favorable where the benefits are larger.
Unfortunately the “high-risk” strategy of prevention also has some serious disadvantages and limitations. . . . [I]t is palliative and temporary, not radical. It does not seek to alter the underlying causes of the disease but to identify individuals who are particularly susceptible to those causes. Presumably in every generation there will be such susceptibles; and if prevention and control efforts were confined to these high-risk individuals, then that approach would need to be sustained year after year and generation after generation. It does not deal with the root of the problem, but seeks to protect those who are vulnerable to it; and they will always be around.
The potential for this approach is limited—sometimes more than we could have expected—both for the individual and for the population. There are two reasons for this. The first is that our power to predict future disease is usually very weak. Most individuals with risk factors will remain well, at least for some years; contrariwise, unexpected illness may happen to someone who has just received an “all clear” report from a screening examination. One of the limitations of the relative risk statistic is that ...