![]()
SPECIAL EDUCATION FOR YOUNG LEARNERS WITH OTHER HEALTH IMPAIRMENTS
Samuel R. Hodge and Eugene Asola
ABSTRACT
This chapter is structured for teaching young learners with other health impairments in special education. Under the Individuals with Disabilities Education Improvement Act (IDEA, 2004), other health impairments represent chronic or acute health problems such as asthma, attention deficit disorder or attention deficit hyperactivity disorder (ADHD), diabetes, epilepsy, a heart condition, hemophilia, lead poisoning, leukemia, nephritis, rheumatic fever, and sickle cell anemia and adversely affect a child’s educational performance. The chapter is organized around definitions, prevalence, etiologies, intervention strategies, and teaching considerations for selected disabling conditions in this disability category.
Keywords: Educational interventions; other health impairments; programmatic modifications; special educators; young learners; school physical education
This chapter is constructed for teaching young learners with other health impairments in special education. Special education is defined in the Individuals with Disabilities Education Improvement Act (IDEA) (IDEA, 2004) as expressly designed instruction, at no cost to parents (or guardians), to address the unique needs of children with disabilities, “including: (a) instruction conducted in the classroom, in the home, in hospitals and institutions, and in other settings; and (b) instruction in physical education” (p. 118, Stat. 2658). In the 39th Annual Report to Congress on the Implementation of IDEA, students aged six through 21 with other health impairments accounted for 15% of those served in 2015 under IDEA, Part B (United States Department of Education [USDE], 2017). Students with physical and other health impairments present both challenges and opportunities to teachers as presented in Chapter 11 of this book. In Chapter 11, the case of Amira, a girl with asthma and cerebral palsy was discussed. The critical question is, how can we ensure that Amira and other students with health impairments participate as fully as possible in general or special education programming?
Other Health Impairments as a category includes young learners who have a medical condition that impedes their education. More specifically, “other health impairments include having limited strength, vitality, or alertness due to chronic or acute health problems such as a heart condition, tuberculosis, rheumatic fever, nephritis, asthma, sickle cell anemia, hemophilia, epilepsy, lead poisoning, leukemia, or diabetes” (McFarland et al., 2017, p. 110). Clearly, the category of other health impairments includes a wide range of conditions extending from conditions with no apparent symptoms to disabling conditions that may result in death (Hodge, Lieberman, & Murata, 2012).
This category is situated in Public Law 101-476 of the IDEA. The reauthorized Individuals with Disabilities Education Improvement Act (2004) define other health impairment as:
[…] having limited strength, vitality or alertness, including a heightened alertness to environmental stimuli, that results in limited alertness with respect to the educational environment, that is due to chronic or acute health problems such as asthma, attention deficit disorder or attention deficit hyperactivity disorder, diabetes, epilepsy, a heart condition, hemophilia, lead poisoning, leukemia, nephritis, rheumatic fever, and sickle cell anemia; and adversely affects a child’s educational performance.” (34 Code of Federal Regulations §300.7(c)(9))
It is clear from the aforementioned definition that many ailments may impact a child’s health as well as opportunity and ability to learn. Most health impairments are chronic ailments which are always present and may even recur. For services under IDEA’s other health impairments category, the child’s health condition must limit strength, energy, or preparedness to such a degree that his or her education is negatively affected (Pierangelo & Giuliani, 2007). In deciding on whether or not a child qualifies for special education services under other health impairments, the following questions should be asked (see Hodge et al., 2012; Pierangelo & Giuliani, 2007):
- Does the child have a chronic or acute health problem?
- Does the child have limited strength, vitality, or alertness?
- If so, does the child’s limitations reduce her or his learning?
- If so, is the child’s educational performance negatively affected by these limitations?
- Finally, does the child’s disability create a need for special education services?
Additionally, the varying types of other health impairments can be categorized into the following general areas: allergies, heredity, accidents, multiple factors, and unknown (Pierangelo & Giuliani, 2007). Moreover, the general behavioral tendencies faced by learners with other health impairments include attention, coordination difficulties, fatigue, mobility issues, muscle weakness, frequent absences or lateness to school, stamina, and concentration (Hodge et al., 2012). Other health impairments affect youth from all cultures and socioeconomic backgrounds (Pierangelo & Giuliani, 2007).
DIABETES MELLITUS: TYPES 1 AND 2
Diabetes mellitus is a chronic disease associated with abnormally high levels of sugar or glucose in the blood. In this disease, the body cannot properly burn the glucose (body fuel) it gets from food for energy (Nieman, 2003). Type 1 (juvenile) diabetes (insulin-dependent diabetes mellitus) requires that the person supplement insulin since the body is unable to produce insulin. Type 1 symptoms include frequent infections, blurred vision, cuts and bruises that are slow to heal, tingling and numbness in extremities, recurring skin, and gum or bladder infections (Nieman, 2003). Type 2 diabetes (non-insulin-dependent mellitus) is the most common type of diabetes. Symptoms consist of any type 1 symptoms that include frequent urination, unusual thirst, hunger, unexplained weight loss, fatigue, and irritability (Nieman, 2003). Type 2 diabetes has commonly been referred to as adult onset diabetes; but, the start has also been found in childhood. Being overweight or obese without a doubt increases the risk of type 2 diabetes. Consequently, type 2 diabetes is often associated with individuals who are obese. While type 2 diabetes is not dependent on continuous insulin injections as is usual with type 1, some form of insulin therapy may be used by those with type 2 diabetes to maintain adequate glucose levels (American Diabetes Association, 2018b).
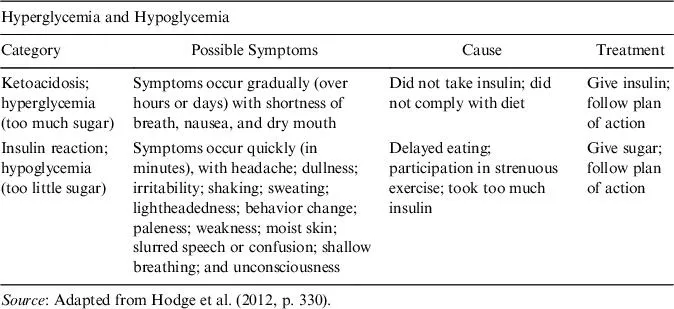
There are three early warning signs for diabetes: (1) polyuria, which means excessive urination, (2) polydipsia, which means excessive drinking, and (3) polyphagia (excessive eating) or anorexia (lack of appetite) (Heller, Alberto, Forney, & Schwartzman, 1996). In regard to polyuria, the body attempts to excrete glucose through the urine as a waste product. In the case of polydipsia, the individual tends to drink excessive amounts of fluids. Since the cells are not getting enough energy, the person may become excessively hungry and eat in excess (Heller et al., 1996). In fact, whether it is polydipsia or anorexia, unexplained weight loss occurs. Further, teachers and related professionals should be mindful that children with diabetes have the potential to have reactions associated with too much insulin or too much glucose (Table 1).
Table 1. Reactions by Too Much Insulin and Too Much Glucose.
The prevalence of diabetes is increasing globally (World Health Organization, 2016). In 2015, there were some 30.3 million people of all ages who had diabetes, which represents 9.4% of the population in the United States (US) (CDC, 2017b). Diabetes is a major health problem that affects some 193,000 Americans under 20 years of age. In addition, it is estimated that over 84 million Americans aged 18 and older had prediabetes in 2015 (American Diabetes Association, 2018c), a condition in which blood glucose levels are higher than normal but are not high enough for a diagnosis of diabetes. People with prediabetes are at increased risk for developing type 2 diabetes and for heart disease and stroke. Other names for prediabetes are impaired glucose tolerance and impaired fasting glucose. Empirical data show that compared to White Americans, the age-adjusted prevalence of diagnosed and undiagnosed diabetes is higher among Asian, Black, and Latina/Latino Americans (CDC, 2017d). More specifically, 7.4% of White adults have been diagnosed with diabetes compared to 8.0% of Asian, 12.1% of Latina/Latino, and 12.7% of Black Americans. Prevalence data further reveal that over 15% of American Indians and Alaskan natives are likely to have been diagnosed with diabetes (American Diabetes Association, 2018c). Young learners from culturally and linguistically diverse backgrounds are more likely to develop type 2 than type 1 diabetes (Spanakis & Golden, 2013). Spanakis and Golden (2013) asserted that these realities have “economic, public health, and health care system implications for these young individuals who develop a chronic condition at such an early age” (p. 9).
It is commonly held that the etiology of diabetes stems from a combination of genetic and environmental factors. Most often, the etiology for type 1 diabetes can be traced to the body’s inability to excrete insulin to process glucose. The pancreas absorbs and breakdown sugars to be used for energy (Tompkins, Soros, Sothern, & Vargas, 2009). An overproduction of insulin is also a concern in diabetes. Although hereditary factors are relevant in diagnosing type 1 diabetes, the complexity of this condition means that heredity is not the only factor (American Diabetes Association, 2018c; Dunn & Leitschuh, 2006). There are various causes of type 2 diabetes. Although the specific etiologies are unknown, “autoimmune destruction of β-cells does not occur” and individuals “do not have any of the other known causes of diabetes” (American Diabetes Association, 2018a, p. S19). Empirical data reveal that most individuals with type 2 diabetes are overweight or obese (American Diabetes Association, 2018a).
Intervention Strategies
Although there is no one diabetes management formula that fits all young learners (Kaufman, Gallivan, & Warren-Boulton, 2009), there are some basics to follow. Table 2 presents four basics of diabetes management, which include the individual with type 1 diabetes “eating healthy, being active, taking insulin, and tracking blood sugar” (Novo Nordisk, 2017, p. 4). These basics suggest that individuals with diabetes should monitor and care for their diabetes daily. Intervention strategies for insulin-dependent diabetes consist of medication, diet, and exercise (Tompkins et al., 2009). For some, following a very strict regime in taking prescribed medications is required. A prescription of the amount of insulin needs to be written by a physician; and monitoring of blood glucose levels should be completed first, before injecting insulin into the body. The insulin is injected into the body at specific areas: arms, waist line, and upper thighs (Petray, Fresseman, & Lavay, 1997).
Table 2. Basics of Diabetes Management.
Healthy eating: Maintaining the habit of healthy eating comes from creating balance, and meal plans can include many options and flavors. For the child with type 1 diabetes, it’s essential to keep track of foods eaten and adjust insulin dosing accordingly. The child’s healthcare team can help one forge a plan that works | Being active: Physical activity gives the child with type 1 diabetes more energy and makes his or her body more receptive to insulin. These are good things, but with type 1 diabetes, it’s important to monitor blood sugar with activity. Also one must consider keeping “emergency carbs” on hand, like fruit juice, glucose tablets, or hard candies |
Taking insulin: The child with type 1 diabetes is likely to have been prescribed a daily basal-bolus insulin therapy, taken either by pump or injections, that involves both a long-acting (basal) insulin and a rapid-acting (bolus) insulin that closely mimics the body’s normal insulin release. With type 2, treatment options will vary with the individual needs o... |