![]() Section 1
Section 1
Regenerative Medicine:
From Historic Developments
to State-of-the-Art Therapies![]()
1
Aspects of Tissue Engineering and Regenerative Medicine in Maxillofacial Reconstruction
Geoff McKellar*, Ann Collins†
Oral and Maxillofacial Surgeons
*Westmead Hospital and the Children’s
Hospital, Sydney, Australia
†University of Sydney, Australia
1.1 Introduction
In all living creatures, Urist3–5, 82–84 proposed that “development begins in a morphogenetic way and ends in a cytodifferentiation phase. In the first half of the 20th century, cytodifferentiation was the principal problem of bioscience. Now the problem has become morphogenesis and is generally viewed as the covert phase, while cytodifferentiation is an overt phase of development. The morphogenetic phase activates a genetic programme for the arrangement of species specific extracellular substances. The cytodifferentiation phase is instituted by the differentiation of specialised cells.”1 This is highly relevant to the development of the head and neck with its complex multiple anatomical compartments. Turing expressed the kinetics of morphogenesis in mathematical terms and designated molecules initiating reactions which connect the phenotype to the genotype.2 Conceptually, morphogens promote a genetic programme for the development of the three-dimensional form and structural features of the organism. One morphogen named bone morphogenetic protein (BMP) has been isolated and biosynthesised by recombinant gene technology.3–7 BMPs today are now available for basic investigations of bone development and treatment of a wide selection of skeletal disorders. The adjective “morphogenetic” was interpreted to mean that the BMP generates from a three-dimensional structure of a bone complete with a marrow cavity and functioning haematopoietic bone marrow containing mesenchymal stem cells (MSCs). These cells are self-renewing, multipotent precursors which were originally found to reside in the stromal adherent fraction of the bone marrow, where they sustain the homeostatic turnover of non-haematopoietic stromal cells, regulate haemopoetic stem cells (HSCs) maintenance and contribute to vascular stability. MSCs can be expanded in vitro to generate mesenchymal stromal cell cultures which, under appropriate conditions, can differentiate into adipocytes, chondrocytes and osteoblasts. Multipotent mesenchymal stromal cell cultures have been derived from perivascular stem cells expressing pericyte markers in many postnatal tissues. The differentiation capabilities, paracrine potential and ease of isolation of in vitro expanded mesenchymal stromal cells have contributed to the exploitation of MSCs as therapeutic agents for tissue regeneration and repair.
The principles of tissue engineering include:
- Morphogenetic signals.
- Responding stem cells.
- Extracellular matrix scaffolding.
We are entering a new era of regenerative medicine in which patients and the healthcare system will see derived benefits from faster and more predictable clinical healing using less invasive treatment modalities and recombinant protein therapeutics which continue the major evolution in our regenerative therapies. Doctors now have access to pure recombinant tissue growth factors, allowing them to progress patterns of healing, thereby enhancing the opportunities for the regeneration of bone and other tissues.54
Tissue regeneration using platelet-rich plasma (PRP) or recombinant protein therapeutics and biodegradable scaffolds are now able to be employed in the healing of clinical craniomaxillofacial and orthopaedic surgical defects. Our understanding of the biological and physical requirements to achieve predictable regeneration of specific tissues will continue to evolve as we establish more optimal binding and release characteristics for the bioactive proteins, more conductive cell scaffolds, and increased use of stem cells.
The clinical cornerstones of craniomaxillofacial reconstruction are the development of a capillary network and regeneration of native tissues together with the functional integration and exteriorisation of prosthetic devices.
Today’s gold standard in clinical practice still remains, for large facial defects, the free vascular transfer of composite tissues together with osseo-integrated components for prosthetic reconstruction.74
1.2 Historical Developments Adapted to Aid Maxillofacial Reconstruction
Globally, early in the 20th century, studies on maxillofacial wound healing were progressed significantly as the result of the clinical demands for patients from the two great wars. There
Fig. 1.1 Reconstructed mandible with osseo-integrated dental implants.46–48
Fig. 1.2 Left mandibular reconstruction with a free vascular fibula graft and dental implants.74
was a progression of understanding of the physiology of the end capillary loop in relation to tissue healing and to the variations of repair of skeletal fractures together with an increased knowledge of local and regional soft tissue flap repair of critical sized wound defects (Figs. 1.1, 1.2). A critical size defect (CSD) is of a dimension that cannot support a free graft without excessive cell death. A CSD may be defined as the smallest size intraosseous wound in a particular bone and species of animal that will not heal spontaneously during the lifetime of the animal.40
1.2.1 Gavril Ilizarov: Distraction osteogenesis 52,53
Ilizarov discovered that by carefully severing a bone without severing the periosteum around it, one could separate the two halves of the bone and fix them in a position such that the bone would grow to fill the gap. He discovered that bone regrows at a fairly uniform rate in the repair of the human skeleton. His experiments led to the design of what is known as an Ilizarov distraction apparatus. It held the severed bone in position by virtue of a framework with pins through the bone and separated the halves of the bone by a tiny amount. By repeating this over
Fig. 1.3 Anatomic biomodel with distraction (Anatomics).
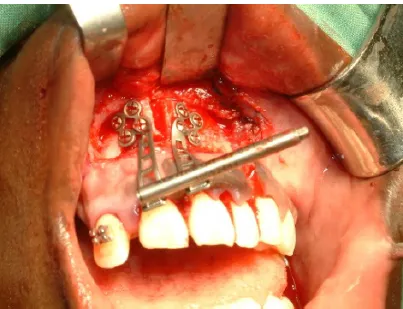
Fig. 1.4 Segmental maxillary alveolar distraction.
time, at the rate of the bone’s regrowth, it was possible to extend the bone by a desired amount. Notably, not only was the bony hard tissue extended, but the soft tissue was also expanded and the adjacent nerve supply remained unaltered. This was a similar discovery to the orthodontic understanding made by Angle at the beginning of the 20th century, that with light forces, teeth could be moved through bone and retain their vitality. This allowed for the modern development of orthodontic treatment.70,71
Further, the concepts of Ilizarov have now been translated to the craniofacial region to help provide solutions to previously unanswered surgical defects and congenital deformities (Figs. 1.3, 1.4).75–77
1.2.2 Marshall Urist: Bone morphogenic protein and platelet-rich plasma 3–5,13,14,83,84
Urist explored the mechanisms of bone growth, development and repair. In particular, based on bone extracts, he discovered a “morphogenetic property” of decalcified bone matrix which acted as a growth factor to stimulate bone formation in a variety of tissues (e.g. subcutaneous tissue, brain, spinal cord, tendon and peritoneum) but not in others (e.g. thyroid, thymus, spleen, liver, kidney).13 Growth factors had been known for decades: in the late 18th century, the term was occasionally used in botany literature to describe external factors (e.g. light, soil nutrients) contributing to growth, but in the 1920s and 1930s, the term was applied in its more curr...