![]()
Case 1
This 58-year-old man was involved in a car-jacking incident and suffered minor trauma to his limbs with bruising and skin abrasions. A cardiologist was asked to provide a medico-legal report on his health as the patient had been found to have an irregular pulse by his general practitioner.
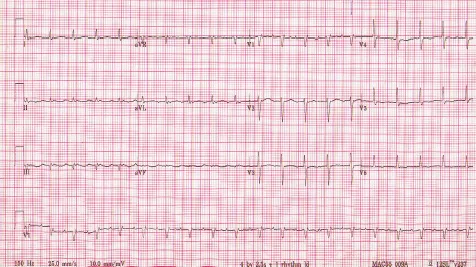
During the consultation, the patient admitted to having become progressively more breathless on exertion over the past 18 months and had noticed some ankle swelling in the past six months. On examination, he had an irregular pulse and a tachycardia of 120 bpm. The jugular venous pressure was elevated to the angle of the jaw and he had marked hepatomegaly and bilateral leg oedema extending to just below knee level. There was reduced air entry at both lung bases. The ECG and chest X-ray are shown below. There was no significant past medical history except that he had been stabbed in the chest at the age of 15 years.
Q
Questions:
1. What does the ECG show?
2. What does the chest X-ray show?
3. What initial treatment should be given?
4. What other investigation should be ordered?
A
Answers:
1. Cardiomegaly, pulmonary venous congestion, bilateral pleural effusions (right > left).
2. Atrial flutter with 2:1 block.
3. In-hospital bed rest, diuretics (intravenous or oral) and a rate controlling agent such as digoxin. Anticoagulant therapy should be commenced.
4. Echocardiography—to assess right and left ventricular function/ size, valve function, atrial size, presence/absence of septal defects or pericardial disease.
The echocardiogram was unremarkable and did not show any evidence of valvular disease or septal defects.
Q
Question:
5. What further imaging test might be helpful?
A
Answer:
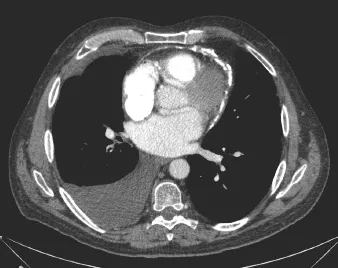
5. CT scan of the thorax.
The CT scan is shown here.
Q
Questions:
6. What does the CT scan show?
7. What is the diagnosis?
8. What other investigation should be organised and what five characteristic features would confirm the diagnosis?
9. What treatment is appropriate?
A
Answers:
6. Dense pericardial calcification and right-sided pleural effusion.
7. Calcific constrictive pericarditis.
8. Cardiac catheterisation of the right and left heart (after stopping anticoagulants).
(i) Elevated right and left atrial pressures, elevated right and left ventricular end-diastolic pressures.
(ii) Equalisation of RV and LV diastolic pressures; equalisation of RA and LA pressures.
(iii) Rapid X and Y descent in RA and LA pressure trace.
(iv) Typical “dip and plateau” waveform in RV and LV pressure recording.
(v) Increase in RA/LA/RVedp/LVedp with inspiration.
9. Pericardiectomy.
![]()
Case 2
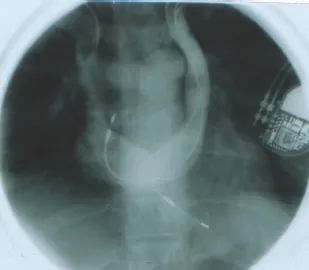
This 40-year-old man presented with left praecordial chest pain which was not regularly related to exertion. There were no abnormalities on physical examination and his resting ECG was normal. An exercise stress test produced–1.3 mm of upsloping ST-segment depression in V5 and V6 at a heart rate of 156 bpm in the third stage of a Bruce protocol. Diagnostic cardiac catheterisation was performed. Simultaneous injections into the right and left coronary artery (left lateral view) are shown below.
Q
Questions:
1. What is the diagnosis?
2. What conclusions can be drawn from the investigation?
A
Answers:
1. Anomalous left circumflex coronary artery, originating from an ectopic, non-dominant right coronary artery.
2. The symptoms are not due to coronary artery disease. The exercise test should be regarded as a negative test.
![]()
Case 3
A 60-year-old man required permanent pacemaker implantation.
Q
Questions:
1. What investigation has been performed here?
2. What abnormality is shown?
3. What specific precautions should be taken during the implantation procedure?
A
Answers:
1. Simultaneous contrast venography from catheters inserted into the right and left arms.
2. Right- and left-sided superior vena cava are present, only discovered during implantation of the first lead which took an abnormal course on fluoroscopy.
3. The pacemaker electrodes should be active fixation leads (particularly the atrial lead) in order to reduce the likelihood of lead displacement post-procedure.
![]()
Case 4
A 74-year-old man presented with dyspnoea and fever of 38.8°C. The chest X-ray and CT scan are shown below.
Q
Questions:
1. What do the chest X-ray and the CT scan show?
2. What is the diagnosis and the likely cause?
3. What two investigations would you perform to confirm the diagnosis?
4. What is the treatment?
A
Answers:
1. The chest X-ray shows a permanent pacemaker with atrial and ventricular leads and a ring-shaped opacity in the left mid-zone.
The CT sca...