![]()
Chapter 1: Diagnosis and Definition
Martin Buysschaert*, Vanessa Preumont,† Jose Luis Medina‡ and Michael Bergman§
Diabetes mellitus is a metabolic disorder of multiple etiologies. Specifically, type 2 diabetes is characterized by chronic hyperglycemia together with disturbances of carbohydrate, fat, and protein metabolism. This condition results from defects of insulin secretion, insulin action, or both, as a consequence of a combination of genetic predisposition, unhealthy diet, physical inactivity, and increased weight.1,2 Type 2 diabetes is a growing public health challenge globally with an estimated prevalence of the disease in 285 million people (corresponding to 6.4% of the world’s adult population), which is expected to reach more than 550 million (7.8% of the population) by 2030, according to recent projections of the International Diabetes Federation (IDF). Of the total, 70% of these cases occur currently in low- and middle-income countries.3,4 Long-term hyperglycemia in type 2 diabetes is associated with progressive damage of various organs, including eyes, kidneys, nerves, heart, and blood vessels, with premature mortality and has considerable economic impact.2
Prior to the development of type 2 diabetes, glucose levels can increase in a prediabetic state that may exist for many years before type 2 diabetes comes to be diagnosed.5,6 Dysglycemia is characterized by higher glucose levels than normal but lower than defined by conventionally established thresholds for diabetes. Globally, prediabetes should not be viewed as a clinical entity but rather a risk factor for diabetes development as well as for cardiovascular disease. This high-risk prediabetic state includes isolated impaired fasting glucose (IFG), isolated impaired glucose tolerance (IGT), or combined IFG/IGT.7 The prevalence of IFG/IGT increases with age as indicated in the DECODE Study (IGT increased from 3.9% in 30 to 39-year-old men to 15.1% in the 70- to 79-year-old age group and from 4.5 in 30- to 39-year-old women to 16.9% in the 70- to 79-year-old age group).8 It has been predicted that globally there will be 470 million people in 2030 with prediabetes.4
Diagnosis of prediabetes is mandatory since numerous clinical studies have confirmed that a substantial number of individuals with this disorder will later develop diabetes with an average annual risk approximating 5–10% compared with below 1% in normoglycemic subjects.9–11 Furthermore, IFG/IGT is also associated with microvascular complications, neuropathy, and cardiovascular disease.12–15 Kurihara et al. recently showed that coronary atherosclerosis and plaque vulnerability were more advanced in patients with prediabetes than those without diabetes and were comparable between individuals with prediabetes and diabetes.16 Therefore, early recognition is crucial as lifestyle modification as well as medications have been shown to be effective, particularly in reducing progression to diabetes.7,17–19
Diagnosis of IFG/IGT is an evolving process as cutoff values have been revised several times in the past decades as new research data became available. Along this line, the aim of this chapter is to review the past and present definitions of prediabetes, including the place of HbA1c as a diagnostic procedure.
1. THE PAST HISTORY OF “GLUCOSE INTOLERANCE”
Before 1979, a state of “borderline” diabetes had been recognized by the World Health Organization (WHO)’s First Expert Committee when there was uncertainty about the diagnosis of diabetes, but where blood glucose levels were above normal.20
The National Diabetes Data Group (NDDG), in 1979, confirmed that a raised blood glucose was the hallmark of diabetes but was also the first to introduce the concept of a prediabetic condition referred to as “glucose intolerance,” defined as a metabolic (hyperglycemic) state intermediate between normal glucose homeostasis and diabetes.21 The NDDG indicated that a 75 g load of glucose would be appropriate for diagnosis of both conditions when consumed in 300 mL water over 5 m (when at least 250 g carbohydrates were consumed for 3 days before the test). The fasting and 2-hr values diagnostic criteria for diabetes were largely established on the basis of predicting the development of retinopathy.22 Briefly, diabetes was defined by a fasting plasma glucose (FPG) equal to or greater than 140 mg/dL (7.8 mmol/L) (on more than one occasion) or on a 2-hr value after a 75 g oral glucose tolerance test (OGTT) equal to or greater than 200 mg/dL (11.1 mmol/L) and at another time between 0 and 2 hr. Diabetes was also diagnosed in the presence of an “unequivocal” elevation of plasma glucose with classical signs and symptoms of hyperglycemia. In the NDDG report, “glucose intolerance” by itself was identified by the simultaneous presence of three criteria: a FPG level lower than 140 mg/dL (7.8 mmol/L), a glucose value between 140 and 199 mg/dL (7.8–11.0 mmol/L) 120 m after an OGTT, and at least one other glucose concentration equal to or exceeding 200 mg/dL (11.1 mmol/L) at 30, 60, and 90 m during OGTT (Table 1). These criteria were established in 1980 by the WHO, which stated, however, that glucose intolerance could be defined after OGTT by a single glucose level between 140 and 199 mg/dL (7.8–11.0 mmol/L) at 120 m if the FPG was below 140 mg/dL (7.8 mmol/L) (i.e., two criteria for “glucose intolerance” in the WHO vs. three in the NDDG).23 In 1985, the WHO group adjusted their fasting and post-challenge values to precisely match the NDDG criteria.24
2. THE MODERN ERA OF “PREDIABETES”
2.1. Step 1
An International Expert Committee (IEC) convened by the American Diabetes Association (ADA) and IDF, in 1997, and the WHO, in 1998, re-examined the diagnostic criteria of (pre)diabetes in light of new epidemiological data available since the princeps NDDG report.25–27 One objective was to make the FPG and the 2-hr glucose value during OGTT equivalent for diagnosing diabetes: thus if one criterion was met, the other would likely be met as well. In this view, the IEC recommended that the FPG threshold for diagnosing diabetes be reduced from 140 to 126 mg/dL (7.8–7.0 mmol/L). The IEC linked the new levels with cross-sectional data showing that the risk of development of retinopathy already begins at approximately 126 mg/dL (7.0 mmol/L) in the fasting state in several cohorts, including Egyptians, Pima Indians, as well as a group of the Third National Health and Nutrition Survey (NHANES III).25,28,29 The 2-hr glucose cutoff point for diagnosing diabetes after an OGTT remained unchanged as equal to or greater than 200 mg/dL (11.1 mmol/L), as well as based on the presence of clinical symptoms and measurement of a casual plasma glucose level equal to or greater than 200 mg/dL (11.1 mmol/L) (Table 1). It is of interest, however, that with the reduction of FPG threshold to 126 mg/dL (7.0 mmol/L), it was thought that it was no longer necessary to perform an OGTT in all individuals in order to diagnose those with diabetes.
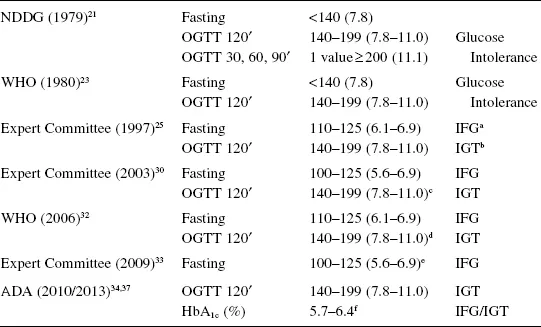
Table 1. Diagnostic criteria for prediabetes: historical synopsis.
Notes : Plasma glucose levels are expressed in mg/dL (mmol/L).
a IFG for impaired fasting glucose.
b IGT for impaired glucose tolerance.
c OGTT not recommended.
d OGTT recommended.
e 110–125 (6.1–6.9) for the WHO.
f WHO does not make any formal recommendation on the interpretation of HbA1c <6.5% in terms of prediabetes.
As far as the prediabetic state was concerned, both the IEC and WHO introduced the concept of IFG as a fasting plasma glucose above norma...