![]()
Operative Procedure
Before the first incision is made, adequate preparation is necessary to ensure a smooth operation. This process is usually protocoled, and ensures that the correct operation is being performed on the correct patient. In addition, the surgeon must check that all necessary equipment is set up and available before initiating the operation. Rushing to begin the operation without ensuring proper set-up compromises the safety of the patient, and usually leads to unnecessary angst and stress for the surgical team.
Positioning of Patient
Patients are placed in a supine position, usually with the right arm tucked in and flushed against their torso. Their left arm can be tucked in also, but is usually positioned at right angles to the torso on an arm-board to provide easier intravenous access for the anaesthetist. The right arm is tucked in specifically to provide for standing space for the assistant in the event of a conversion to open surgery. This allows for the surgeon to operate from the right side of the patient, with additional space to the surgeon’s left for an assistant to perform retraction of the right costal margin.
Warming mats placed beneath the patient are routinely used in most institutions to mitigate heat loss from the patient during the operation. Warmed air insufflators to create a cushion of warm air between the sheets and the patient’s lower limbs are used for the same effect.
The supine position is the most benign due to the relative lack of created pressure points that may increase the risk of pressure sores. The relative short duration of a laparoscopic cholecystectomy also safeguards against the development of any iatrogenic pressure sores intra-operatively.
Cleansing and Draping
As per all abdominal operations, patients are cleaned from nipple level to mid-thigh. We prefer chlorhexidine-alcohol preparations, though iodine-based preparations have the advantage of delineating clearly the areas that have been cleansed. In particular, the right side of the abdomen should be cleansed laterally to the junction of the patient’s body and the bed. This includes the abdominal wall involved in a Kocher’s incision in the sterile field, so additional cleansing is not required in the event of conversion to an open procedure.
The cleanliness of the umbilicus for any laparoscopic procedure cannot be over-emphasised. Due to personal hygiene practices (or the lack thereof) and/or body habitus, the umbilicus is a common repository of debris consisting of sloughed keratin, clothing fabric and microorganisms. Cotton-tipped sticks dipped in chlorhexidine are commonly used in clearing deep-seated debris, and alcohol swabs can be used for flatter navels. Failure to pay proper attention to the sterility of this area significantly increases the risk of surgical site infection at the peri-umbilical incision.
Drapes should expose just the top of the costal margin and the xiphoid process, whilst extending to the right laterally to the mid-axillary line. This facilitates the placement of the lateral most laparoscopic port. It also allows for a lateral Kocher’s (subcostal) incision that may be required in complex converted cases. The inferior edge of the drapes should be at least 2 cm below the umbilicus, which allows for enough space even if a sub-umbilical incision is made for the insertion of the laparoscope.
Positioning of Surgeon, Assistants and Camera System
High-definition television systems have become the norm in most laparoscopic procedures, with a number of manufacturers providing comparable products. An in-depth account of camera system workings is detailed in the Appendix.
The television monitor is positioned to the side of the patient’s right shoulder, tilted towards his/her right hypochondrium. This allows for a straight line between the surgeon, area of interest (right hypochondrium) and the monitor, for improved ergonomics.
The surgeon stands on the left side of the patient, just below the level of the umbilicus, with his body tilted towards the patient’s right hypochondrium and facing the video monitor. From this spot, he is well positioned to control both working ports.
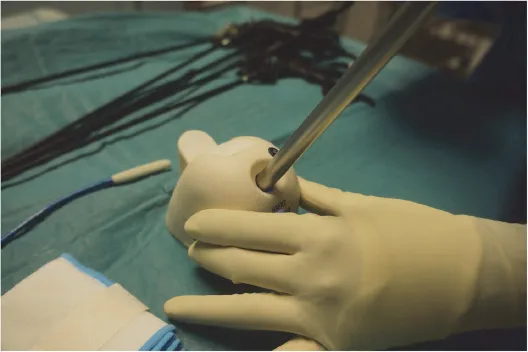
The camera assistant stands just behind the left shoulder of the surgeon, often having to manipulate the laparoscope from a slightly awkward position so as to stay clear of the surgeon’s left arm. The camera assistant usually holds the camera head base with his/her right hand from below, with his/her left hand toggling the fibre-optic cable to manoeuvre the viewing perspective, and to capture images by operating the controls on the camera head. In the case of a coaxial camera head system, both hands are also needed to control the up-down and left-right dials on the camera head (Fig. 1).
Fogging of the laparoscope lens is a common source of hindrance for the surgical team. It is primarily caused by the condensation of warmer water molecules present in the peritoneal cavity onto the colder surface of the lens. This can be somewhat mitigated by pre-heating the laparoscope in a special heating unit that is part of most camera systems. We find the use of a sterile thermo-flask filled with near boiling water for intermittent warming of the laparoscope during the operation very effective. A piece of gauze is placed at the bottom of the flask to prevent scratch injury to the delicate laparoscope lens.
Figure 1.Positioning during surgery. The patient is lying supine with the head further from the foreground. (A) is the surgeon, standing on the left side of the patient facing the patient’s right shoulder. (B) is the camera assistant. (C) is the first assistant providing cephalic retraction of the gallbladder. (D) is the scrub nurse.
Anti-fogging solutions that are applied to the lens by way of a sponge are also readily available, but not as successful in our experience. Intraoperatively, the gentle rubbing of the angled laparoscope lens on the liver surface can also be attempted to clear the condensation; this method becomes considerably less successful however, once the liver surface is itself covered with a layer of oil and water from the adjacent cautery. Newer anti-fogging devices have been developed which allows for intra-operative warming and cleansing of the telescope lens by way of a battery-operated docking system, which we have used with some success (Fig. 2).
The first assistant stands on the right side of the patient at approximately the level of the camera assistant, if needed. His/her main purpose for the majority of the operation is to retract the gallbladder over the inferior edge of the liver. His/her grip on the gallbladder should remain still, and should only move the gallbladder when directed by the surgeon. Pressing the shaft of the grasping forceps against the patient’s body with the left hand, while the right hand grips the instrument handle firmly can attain additional leverage in lifting the gallbladder over the liver. A piece of gauze placed strategically between the instrument port and the patient’s skin helps to avoid pressure injury.
Figure 2.Intra-operative warming and cleansing of the laparoscope.
Creation of Pneumoperitoneum
The initial incision is made in the peri-umbilical region; depending on surgeon preference, this can be trans-umbilical, supra-umbilical or infra-umbilical. We prefer a 10 mm curved infra-umbilical following the circumference of the navel, for cosmesis and ease of wound closure and dressing. The skin is stretched lightly with the help of the non-dominant hand, and the incision made to breach the dermis (Fig. 3).
The subcutaneous fat, Camper’s fascia and Scarpa’s fascia are bluntly cleared with a pair of artery forceps. The non-dominant hand maintains an opening in the tissues with its artery forceps’ jaws open, whil...