![]()
1
Diabetic Foot Wounds — Types of Wounds and Classification Systems
Aziz Nather and Tan Ting Fang
Introduction
Diabetes currently affects 387 million people globally, and it is expected to increase to 552 million by 20301 or one in ten adults (Fig. 1), owing to environmental factors such as sedentary lifestyles and changing dietary patterns. Ranked in the top ten leading causes of death in the world,3 diabetes has been considered as the “global epidemic of the 21st century”.
Foot ulcers are very common in diabetic patients. It affects 15% of diabetic patients and precedes 84% of diabetic-related lower limb amputations.4 A diabetic patient is 40 times more likely to receive a lower limb amputation.4 Currently, it is estimated that for every 20 seconds, a leg is amputated due to diabetes worldwide.5
Lower limb amputations often cause mortality in diabetic patients: 70% of them die within five years after an amputation.4
Pathogenesis
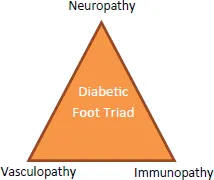
It is necessary to first understand the pathogenesis of diabetic foot ulcers — the “Diabetic Foot Triad” (Fig. 2). The three risk factors — neuropathy, vasculopathy and immunopathy — contribute to varying degrees in different patients.
Figure 1. Diabetic foot triad
Table 1. Global prevalence of diabetes (2014 and 2030)
| | 2014 | 2030 |
| Total world population (in billions) | 7 | 8.3 |
| Adult population (20–79 years, in billions) | 4.4 | 5.6 |
| Number of people with diabetes (in millions) | 387 | 552 |
| Global prevalence of diabetes (%) | 8.3 | 9.9 |
In some patients, one component predominates (e.g. dry gangrene due to ischaemia), a combination of two risk factors may be responsible in others (e.g. wet gangrene due to ischaemia and infection). On the other hand, all three factors — neuropathy, ischaemia and infection — may be present in some patients.
Types of Wounds
Infective Wounds
Infective wounds are usually found on the dorsum of the foot or in the web space (Fig. 2).
Ischaemic Wounds
Ischaemic wounds result from diabetic vasculopathy (Fig. 3). Signs of chronic ischaemia are (1) shininess of the skin; (2) hair loss; (3) increased skin pigmentation; and (4) trophic nail changes. However, in most diabetic foot ulcers there is a degree of ischaemia, which is not severe enough to be apparent but promotes infection and causes delay in healing and increases risk of amputation.
Figure 2. Infective wounds
Figure 3. Ischaemic wounds
Both Infective and Ischaemic
Some wounds have features of both infection and ischaemia (Fig. 4).
Neuropathic Wounds
Neuropathic wounds usually occur in weight-bearing areas as a result of loss of protective sensation and high pressure points from changes in the mechanics of the foot (Fig. 5).
Figure 4. Both infection and ischaemia present
Figure 5. Neuropathic wounds
Decubitus Wounds
Decubitus wounds occur when too much pressure is constantly placed on the skin. Common sites include the heel, lateral malleolus and the lateral aspect of the 5th metatarsal (Fig. 6).
Classification Systems
For this set of guidelines, we have adopted the Wagner-Meggitt Wound Classification5,6 for classifying the wounds. In addition, the King’s College Classification7 is also used.
Wagner-Meggitt Wound Classification
This classification (Table 2 and Fig. 7) was first described by Meggitt in 19765 and popularised by Wagner in 1981.6 It is a six-grade system that classifies ulcers according to the depth and extent of wound.
The advantages of the Wagner-Meggitt Wound Classification include its simplicity in usage and providing a guide for practitioners to plan the treatment...