![]()
| 2 | Retinal Vascular Disease |
Macroaneurysm
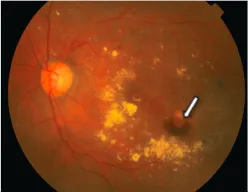
Retinal macroaneurysms are focal fusiform or saccular dilations, typically occurring within the first three bifurcations of the central retinal artery. They are seen predominantly in the elderly above 60 years of age and females are three times more likely to be affected. They are most commonly associated with systemic hypertension and generalized arteriosclerotic disease. Visual loss can be a result of macular exudation and/or hemorrhage into the vitreous, subretinal and intraretinal space.
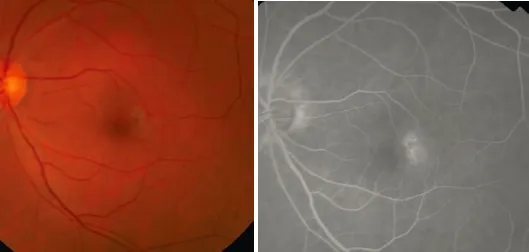
Fig. 2.1.Color fundus photograph of a patient with macroaneurysm (arrow), with surrounding intraretinal hemorrhage, hard exudates and macular edema.
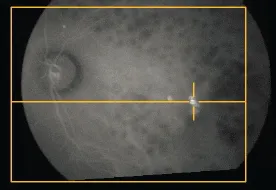
Fig. 2.2.ICG shows a hot spot corresponding to the position of the macroaneurysm on fundus photograph.
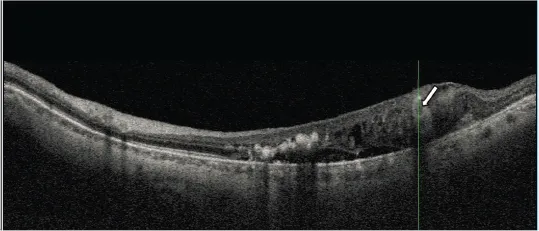
Fig. 2.3.SS-OCT of the above patient. A hyperreflective lesion corresponding to the macroaneurysm is seen within the intraretinal space (arrow).
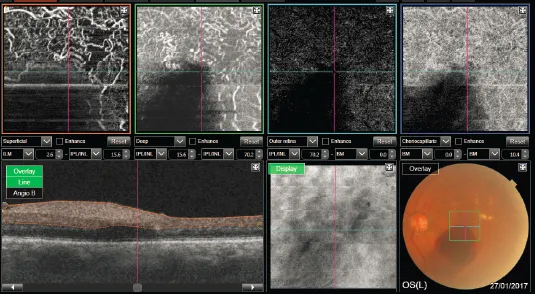
Fig. 2.4.3 × 3 mm OCT-A of a patient with left eye retinal macroaneurysm. The vasculature in all the layers are obscured at the region of hemorrhage. The superficial and deep vascular shows disorganized and tortuous vessels.
Idiopathic Macular Telangiectasia
Idiopathic macular telangiectasia is a group of retinal vascular disorders characterized by retinal capillary dilatation of unknown cause affecting the macula. Macular telangiectasia Type 1 is an aneurysmal telangiectasia associated with exudation, almost always unilateral and affecting men more commonly. Macular telangiectasia Type 2 is a bilateral disease involving the macular capillary network and characterized by atrophy of the neurosensory retina. It typically affects individuals in the fifth or sixth decade of life with no gender predilection. It can be further classified into a nonproliferative stage where there is foveal atrophy, and a proliferative stage with the development of subretinal neovascularization. Table 2.1 shows the stages of macular telangiectasia Type 2.
Table 2.1.Idiopathic Juxtafoveal Retinal Telangiectasis of Gass and Blodi (based on Biomicroscopy and Stereoscopic Fluorescein Angiography).
| Stage 1 | No biomicroscopic abnormality, no or minimal capillary dilation, mild staining of outer perifoveal retina |
| Stage 2 | Slight graying of perifoveolar retina, no or minimal biomicroscopically visible telangiectatic vessels, but capillary telangiectasis of outer capillary network temporally on fundus autofluorescence |
| Stage 3 | One or several slightly dilated and blunted retinal venules descending into outer perifovea, typically temporally |
| Stage 4 | Pigment hyperplasia, often surrounding right-angle venules |
| Stage 5 | Subretinal neovascularization, often in proximity to intraretinal pigment migration |
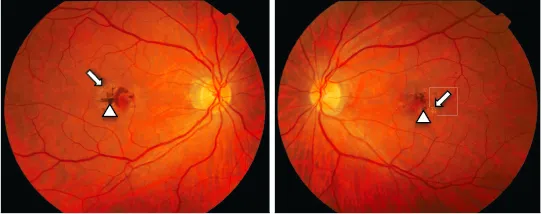
Fig. 2.5.Macular telangiectasia Type 2. Note the presence of bilateral disease affecting the macular, characterized by pigment proliferation (arrowheads) and crystalline deposits (arrows).
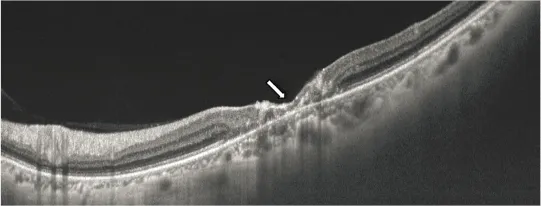
Fig. 2.6.SS-OCT of the right eye shows foveal atrophy (arrow) with loss of the outer retina, representing a late stage of disease.
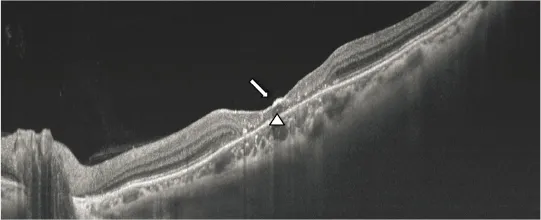
Fig. 2.7.SS-OCT of the left eye shows foveal atrophy (arrow) and the presence of an intraretinal cyst (arrowhead).
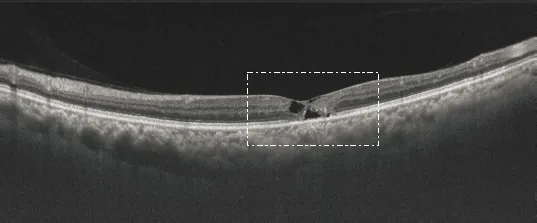
Fig. 2.8.SS-OCT of another patient with macular telangiectasia demonstrating typical cystoid cavities in the absence of macular edema.
Fig. 2.9.Magnified view of the white box above. Note the disruption of the outer retinal layers (arrow). The cystoid cavities are thought to result from dysfunction or lost of muller cells. Crystalline deposits are seen as hyperreflective spots on SS-OCT (arrowhead).
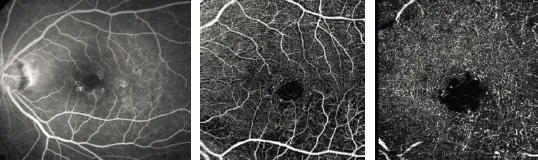
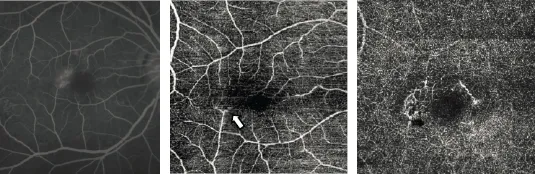
Fig. 2.10a.A 67-year old lady with stage 4 parafoveal telangiectasia of the left eye. Fundal fluorescein angiogram shows diffuse leakage from telangiectatic vessels in the late phase.
Fig. 2.10b.3 × 3 mm OCT-A of the patient in Fig. 2.10a shows disruption and apparent widening of the foveal avascular zone (FAZ) due to intraretinal cysts. Telangiectatic vessels can be seen temporal to the FAZ in the deep capillary plexus (arrow). No choroidal neovascularization is seen in the avascular layer.
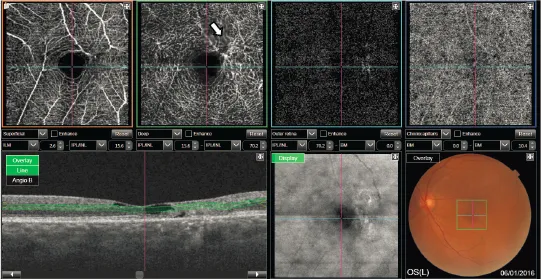
Fig. 2.11.A 67-year-old male with parafoveal telangiectasia of the left eye. Fluorescein angiogram (photo on left) shows leakage from telangiectatic vessels inferior and temporal to the foveal avascular zone. OCT-A of the superficial vascular plexus (middle photo) and deep vascular plexus (photo on right) shows some corresponding telangiectatic vessels. Vessels with slow flow may not be seen on OCT-A.
Fig. 2.12.A 67-year-old female with stage 3 parafoveal telangiectasia of the right eye. Fluorescein angiogram shows leakage from vessels temporal to the FAZ. There is blunting of the retinal vessels (arrow) inferotemporal to the fovea as seen on OCT-A of the superficial capillary plexus (middle photo). Telangiectatic vessels can be seen on OCT-A of the deep capillary plexus.
Retinal Vein Occlusion
Retinal vein occlusion occurs when flow obstruction occurs in either the central retinal vein or one of the branch retinal veins. It is most commonly seen as a complication of hypertensive retinopathy, where the arteriosclerotic retinal arterioles compress the retinal venules at an arteriovenous crossing. It is characterized by intraretinal hemorrhages and exudation in the areas of retina drained by the obstructed vessel. Decreased vision occurs when there is macular edema or significant ischemia. SS-OCT is valuable in visualizing the macula edema, and loss of ellipsoid zone which would suggest a poorer prognosis. Severe ischemia, if left untreated, can result in retinal neovascularization and/or neovascular glaucoma. Evidence from the BVOS and CVOS studies suggested that performing retinal laser photocoagulation to the area of capillary non ...