![]()
The Venous System
![]()
16
Varicose Veins
Introduction
Varicose veins (VV) is a condition which knows no social boundary. Untreated VV is linked to chronic venous hypertension in all strata of society and across all genders; it is a cause of chronic venous insufficiency (CVI) from which untreated VV will produce capillary and skin alterations, pigmentations and venous hypertensive microangiopathy.
This condition when untreated may eventually cause venous ulcerations leading to severe disability, with high personal and social costs. Due to the wide remit of the condition, the problem of VV has been schematically subdivided into primary and secondary categories.
Real or primary VV can be prominent and irregular in caliber, often dysanatomical with normal segments and enlargements and a serpiginous more than a rectilinear course. Secondary veins are usually associated with the consequences of DVT, AV communications, compression of proximal vein trunks increasing distal pressure and pregnancy (in which case most veins may disappear after the end of pregnancy). Dilated veins keep their shape; they appear larger and prominent.
Etiologic factors and distribution
No clear factors — that may be eventually controlled or corrected — have been identified in the development of VV; this multicausal abnormality and clinical condition may evolve into medical problems.
VV are asymptomatic in many subjects for many years. Pain, swelling, edema develop in time with CVI and assume clinical relevance according to individual characteristics and habits; progressive skin pigmentation is associated to long-term presence of CVI.
When veins are prominent, dilated and varicose, superficial thrombosis even from minimal trauma may develop and significant bleeding may occur even with a minor cut. These signs — thrombosis and bleeding — are considered the classic indication for surgical treatment.
Clinical evaluation of the veins (with the patient standing) does not give a complete clinical picture. Inspection may be difficult and misleading. Thermography helps to localize in seconds the most prominent veins (even those that are difficult to see are easily detected by thermography). The presence of thrombotic or inflamed segments is revealed in real time and becomes a target for investigation.
Signs associated with VV and CVI tend to improve with rest, legs elevation and effective elastic compression. Several venous products — mostly of natural origin — effectively control edema and signs/symptoms associated to VV and CVI but have a limited activity of the evolution of the veins and the development of new incompetent segments. These products, usually supplements in pharmaceutical standards (PS supplements), have been evaluated in several studies and appear effective even on the prevention of ulcerations as they control edema.
Most VV are present along the course of the long saphenous vein (LSV) but some veins can be completely separated from the main venous trunks (e.g., linked to a perforating vein). Small reticular veins and telangiectasia may be considered a different disease — more visible when the skin is very transparent — that requires a different, specific management.
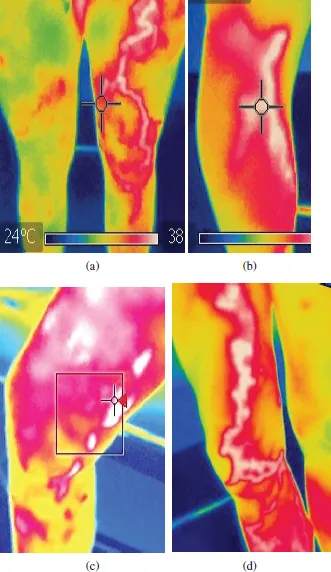
Secondary varicose veins — e.g., following an episode of venous thrombosis or a compression — may be associated to CVI and require a comparable evaluation (usually more complex) and management. Thermographic examples of VV are shown in Fig. 1. Ultrasound Duplex is the primary test to show the localization of reflux in the venous network. The test must exclude arterial problems, thrombosis, venous compressions and deep venous problems (e.g., postthrombotic incompetence).
Figure 1. Patterns of varicosities are revealed and documented in seconds with ultrafast thermography. The increased temperature in some segment may correspond to local thrombosis and may selectively indicate the target for ultrasound assessment. Images also have a medicolegal value, i.e., before and after treatment. Some veins, difficult to see, are clearly shown on thermography.
The evaluation of the superficial venous system must detect the selective competence of the main junctions at first (saphenofemoral junction (SFJ), popliteal — short saphenous vein junction), major, important venous reflux (e.g., longer than 3 s) and minor points of incompetence. Major (high reflow) and minor reflux (lower reflow, reflux lasting <3 s) points can be identified and considered as significant targets for surgery (or sclerotherapy).
The ultrasound evaluation is simple but the anatomy is different from the more regular anatomy of the arteries and requires some experience. Ideally the surgeon treating the veins should test the patient before management.
Treatments
In brief, the treatment of VV is based on finding the major points of incompetence after excluding DVT and deep venous obstruction.
Conservative management
Compression
Elastic stockings below knee are very effective: stockings — with some 25–35 mmHg of compression at the ankle — can be effective in controlling most symptoms and edema. Climatic conditions may alter compliance. Exercise, leg elevation, avoiding the same positions and constricting clothes, weight control may all help in controlling CVI and its consequences.
Increased venous pressure (e.g., due to deep venous incompetence or obstruction) requires higher pressure stocking that tends to decrease compliance. Strong compression stockings take time to wear and cannot withstand heat.
Sclerotherapy
Sclerotherapy can be used in most patients with smaller veins and no major points of incompetence, as the first option. It may also be used as the main option in most patients when surgery is not possible. Also, it is a good, minimally invasive solution for older patients. Smaller veins (caliber <2 mm) and vein segments may be controlled exclusively with sclerotherapy with good, long-term results.
Below-knee veins respond much better to sclerotherapy and compression. Also, vein segments not directly connected with the LSV or other main trunks with higher venous pressure and reflux have, generally, good results with sclerotherapy alone.
Surgery
Stripping may be now considered obsolete: often, most of the veins are only dilated and not incompetent. Resolving incompetence — e.g., at the SFJ — may make most of the remaining veins competent. When ligating the SFJ, it is important to avoid thrombosis of the venous segment close to the ligature of the LSV.
Major points of incompetence, when the diameter of the vein is >2–3 mm, with long reflux (e.g., 3 s with duplex on distal compression-release maneuver) should be treated with surgery when possible. Major points of incompetence also have a hemodynamic value and alter ambulatory venous pressure (AVP) and refilling time (RT) making it much shorter. However, all dilated, prominent or visible veins tend to be associated to incompetence and should be destined to management.
Anatomic veins are easier to identify and classify. Often, nonanatomic veins are present for different causes (e.g., in postthrombotic patients, after previous surgery). These veins should be singularly evaluated and their major incompetence levels (the origin of the reflux) should be identified.
The association of superficial and deep venous incompetence is common. As the possibilities of management for the deep venous system are still limited, the surgeon must aggressively focus on what can be managed in the superficial system. Even a minimal increase in venous pressure (e.g., due to a superficial incompetent segment) may be enough to increase venous pressure and to trigger ulcerations.
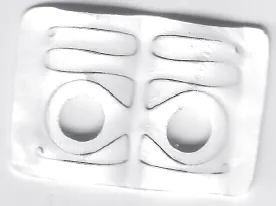
Reconstructive attempts have been made to restore superficial competence. The correction of the most common incompetent site, the SFJ, with a specific external venous valve (EVS, Gore, including a nitinol frame in a Gore-Tex flexible structure) may restore competence in the LSV — in selected subjects — with good results after 10 and 20 years. However, other incompetence points or VV tend to appear as the natural evolution of VV is difficult to slow down (see Fig. 2).
Figure 2. An external valve system (EVS) developed by Gore in Flagstaff, USA, and implanted by us for the first time may keep the vein competent at the SFJ for years. Selected patients may have benefit. The system was particularly useful to study in time (20 years) selective incompetence of venous segments and how this incompetence may propagate to other venous segments. The SFJ is the natural target for this system that — like many other reconstructive methods — was and is limited to a few centers and did not become a common procedure. Costs were relatively high in comparison with ligation or stripping. The Gore-Tex structure includes a nitinol frame that keeps the “memory” of the intended shape of the vein after the implant.
Conclusions on VV therapies
In summary — ideally — the best options for VV are the following:
(a)the surgical treatment (ligation) of the points of major incompetence (particularly proximal to the knee) in association with
(b)sclerotherapy of below-knee veins.
Solutions must be always individualized and applied according to the social context. In many countries, VV surgery is not reimbursed by healthcare providers as it is not considered life threatening. It must be stressed that all methods to control VV are effective in different ways in good hands. When properly and physiologically used, all methods have good, long-term results. The skil...