A concise, quick-reference handbook on history taking and physical examination
Pocket Guide to Physical Assessment is a compact yet comprehensive reference for students and practitioners alike, employing a step-by-step framework for effective patient assessment, diagnosis and planning of care.
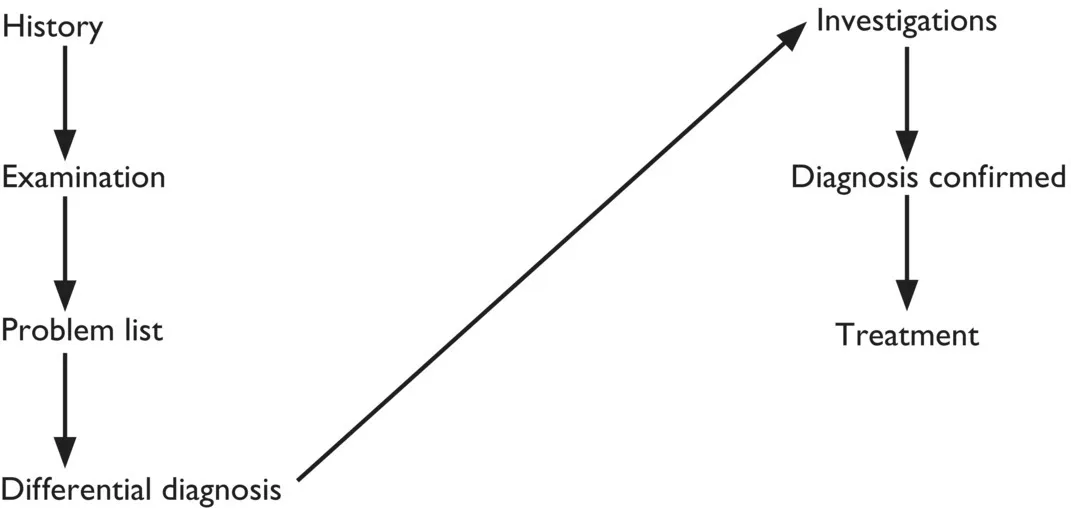
This valuable guide covers topics including cardiovascular, respiratory, neurological and musculoskeletal system examinations, patient interviews, history taking and general health assessments. Clear diagrams and checklists illustrate key points, while easy-to-follow instructions and concise descriptions of clinical situations and diseases aid in clinical decision-making.
- Compact, pocket-sized guide that contains only the essential information for physical assessment
- Instructs readers on best clinical practice and how to present and communicate cases
- Develops and improves necessary skills for physical clinical examinations
- Ideal for use on the ward or as a companion to the accompanying textbook, Physical Assessment for Nurses and Healthcare Professionals
Pocket Guide to Physical Assessment is an invaluable reference for healthcare students, newly qualified and advanced nurse practitioners, and allied health practitioners.