Provides comprehensive coverage of microneedles for delivering and monitoring patient drugs and vaccines
Microneedles are an incredibly active research area and have the potential to revolutionize the way many medicines and vaccines are delivered. This comprehensive research book covers the major aspects relating to the use of microneedle arrays in enhancing both transdermal and intradermal drug delivery and provides a sound background to the use of microneedle arrays in enhanced delivery applications.
Beginning with a history of the field and the various methods employed to produce microneedles from different materials, Microneedles for Drug and Vaccine Delivery and Patient Monitoring discusses the penetration of the stratum corneum by microneedles and the importance of application method and force and microneedle geometry (height, shape, inter-needle spacing). Transdermal and intradermal delivery research using microneedles is comprehensively and critically reviewed, focusing on the outcomes of in vivo animal and human studies. The book describes the important topics of safety and patient acceptability studies carried out to date. It also covers in detail the growing area for microneedle use in the monitoring of interstitial fluid contents. Finally, it reviews translational and regulatory developments in the microneedles field and describes the work ongoing in industry.
The only book currently available on microneedles
Filled with tables, graphs, and black and white images (photographs, micrographs)
Authored by four experts in pharmaceutics
Microneedles for Drug and Vaccine Delivery and Patient Monitoring is an ideal source for researchers in industry and academia working on drug delivery and transdermal delivery in particular, as well as for advanced students in pharmacy and pharmaceutical sciences.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
On the basis of the drug delivery systems, the market can be segmented into eight categories: oral, pulmonary, transdermal, injectable, ocular, nasal, implantable and transmucosal drug delivery. The most common routes of drug delivery are oral, which represent the largest market share (more than 50%), followed by transmucosal (26.2%) and transdermal delivery (12%) [1]. The conventional routes of oral drug delivery have many inherent limitations that could potentially be overcome by advanced drug delivery methodologies, such as transdermal drug delivery (TDD).
The administration of chemical agents to the skin surface has long been practiced, whether for healing, protective or cosmetic reasons. Historically, the skin was thought to be totally impervious to exogenous chemicals [2]. Thus, topical drug therapy typically involved the localized administration of medicinal formulations to the skin, generally when the skin surface was breached by disease or infection and a route of drug absorption into the deeper cutaneous layers was consequently open. However, once it was understood that the skin was a semi‐permeable membrane rather than a totally impermeable barrier, new possibilities arose for the use of this route as a portal for systemic drug absorption.
In the early twentieth century, it was recognised that lipophilic agents had increased skin permeability, and in 1919 the barrier properties of the skin were attributed specifically to the outermost layers [3]. Scheuplein and Blank thoroughly investigated skin permeability to a wide range of substances in vitro [2]. They modelled skin as a three‐layer laminate of stratum corneum, epidermis and dermis, with drug permeation driven by Fickian diffusion. By digesting the epidermal layer, the stratum corneum was separated from the lower layers of the skin and was determined to be the principal barrier to drug absorption.
Transdermal drug delivery refers to the delivery of the drug across intact, healthy skin into the systemic circulation [4]. The diffusive process by which this is achieved is known as percutaneous absorption. The drug initially penetrates through the stratum corneum and then passes through the deeper epidermis and dermis, without drug accumulation in the dermal layer [5]. When the drug reaches the dermal layer, it becomes available for systemic absorption via the dermal microcirculation. Thus, classical topical formulations can be distinguished from those intended for transdermal drug delivery in that, whilst the former are generally applied to a broken, diseased or damaged integument, the latter are used exclusively on healthy skin where the barrier function is intact.
It is, indeed, fortuitous for all of us that the skin is a self‐repairing organ. This ability, together with the barrier protective properties associated with the integument, is a direct function of skin anatomy. Therefore, in order to develop an effective approach to transdermal drug delivery, it is necessary to be aware of how skin anatomy restricts the percutaneous absorption of exogenously applied chemicals.
1.1 Skin Anatomy
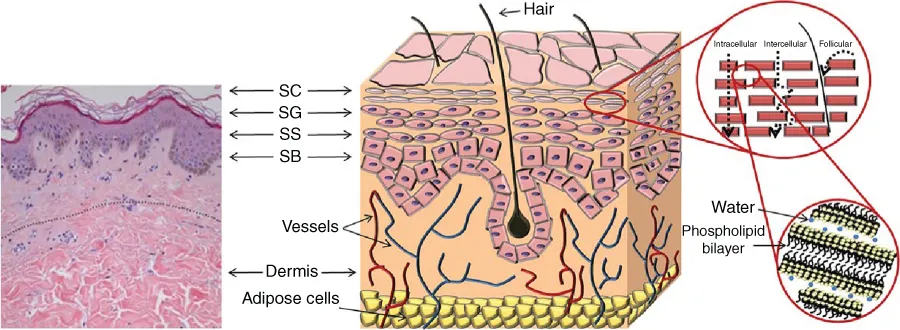
As the largest, and one of the most complex, organs in the human body, the skin is designed to carry out a wide range of functions [6]. Thus, the skin forms a complex membrane with a non‐homogenous structure and a surface area of 1.7 m2, compromising 16% of the total body mass of an average person (Figure 1.1). It contains and protects the internal body organs and fluids, and exercises environmental control over the body with respect to temperature and, to some extent, humidity. In addition, the skin is a communicating organ, relaying the sensations of heat, cold, touch, pressure and pain to the central nervous system.
Figure 1.1 Schematic representation of the skin. Comparison with a histological section of mammary skin from a 19 year old patient (left). From inside to outside, the adipose cells, the dermis (the only vascular layer; thickness 0.3–4 mm; fibroblasts, sweat glands and hair follicles are present), the epidermis (thickness 100–150 μm) composed of stratum basale (SB), stratum spinosum (SS), stratum granulosum (SG), and stratum corneum (SC). Cells differentiate from SB to SC up to lose their nuclei. In the SC cells (corneocytes) are embedded in a matrix of lipid bilayers (brick and mortar model) (right). Penetration routes of molecules are reported with dotted arrows. The number of SC layers depends on the body site, age, skin condition and skin hydration (generally 6–20 but also 86 in the heel). Total thickness of SC is 10–30 μm..
Reproduced with permission from [30] R.J. Scheuplein (1972) Properties of the skin as a membrane. Adv. Biol. Skin. 12: 125–152
1.1.1 The Epidermis
The multilayered nature of human skin can be resolved into three distinct layers. These consist of the outermost layer, the epidermis, beneath which lies the much larger dermis and, finally, the deepest layer, the subcutis. The epidermis, which is essentially a stratified epithelium, lies directly above the dermo–epidermal junction. The viable epidermis is often referred to as the epidermal layers below the stratum corneum. This provides mechanical support for the epidermis and anchors it to the underlying dermis. The junction itself is a complex glycoprotein structure about 50 nm thick [7].
Directly above the undulating ridges of the dermo–epidermal junction lies the basal layer of the epidermis, the stratum germinativum. This layer is single cell in thickness with columnar‐to‐oval shaped cells, which are actively undergoing mitosis. As the name implies, the stratum germinativum generates replacement cells to counterbalance the constant shedding of dead cells from the skin surface. In certain disease states, such as psoriasis, the rate of mitosis in this layer is substantially raised in order to compensate for a diminished epidermal barrier, the epidermal turnover time being as fast as four days. As the cells of the basal layer gradually move upwards through the epidermis, they undergo rapid differentiation, becoming flattened and granular and the ability to divide by mitosis is lost. Directly above the stratum germinativum is a layer, several cells in thickness, in which the cells are irregular and polyhedral in shape. This layer is the stratum spinosum, and each cell has distinct spines or prickles protruding from the surface in all directions. Although they do not undergo mitosis, the cells of thi...
Table of contents
Cover
Table of Contents
Copyright
List of Contributors
About the Editors
Preface
Chapter 1: Genesis of Transdermal Drug Delivery
Chapter 2: Microneedle Manufacturing and Testing
Chapter 3: Microneedle‐mediated Drug Delivery
Chapter 4: Microneedle‐mediated Vaccine Delivery
Chapter 5: Microneedles for Gene Therapy: Overcoming Extracellular and Intracellular Barriers
Chapter 6: Delivery of Nanomedicines Using Microneedles
Chapter 7: Minimally‐invasive Patient Monitoring and Diagnosis Using Microneedles
Chapter 8: Delivery of Photosensitisers and Precursors Using Microneedles
Chapter 9: Microneedles in Improving Skin Appearance and Enhanced Delivery of Cosmeceuticals
Chapter 10: Microneedles for Ocular Drug Delivery and Targeting: Challenges and Opportunities
Chapter 11: Clinical Translation and Industrial Development of Microneedle‐based Products
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Microneedles for Drug and Vaccine Delivery and Patient Monitoring by Ryan F. Donnelly, Thakur Raghu Raj Singh, Eneko Larrañeta, Maeliosa T.C. McCrudden, Ryan F. Donnelly,Thakur Raghu Raj Singh,Eneko Larrañeta,Maeliosa T.C. McCrudden,Maeliosa T. C. McCrudden in PDF and/or ePUB format, as well as other popular books in Physical Sciences & Organic Chemistry. We have over 1.5 million books available in our catalogue for you to explore.