Pharmacovigilance is the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problems.
This introductory guide is designed to aid the rapid understanding of the key principles of pharmacovigilance. Packed full of examples illustrating drug safety issues it not only covers the processes involved, but the regulatory aspects and ethical and societal considerations of pharmacovigilance.
Covering the basics step-by-step, this book is perfect for beginners and is essential reading for those new to drug safety departments and pharmaceutical medicine students. The second edition is thoroughly revised and updated throughout and includes a new chapter on clinical aspects of pharmacovigilance.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1 What is Pharmacovigilance and How Has it Developed?
Origins and Definition of Pharmacovigilance
In the beginning, there was thalidomide. The history of drug safety goes back further but, for practical purposes, the story of modern pharmacovigilance begins there.
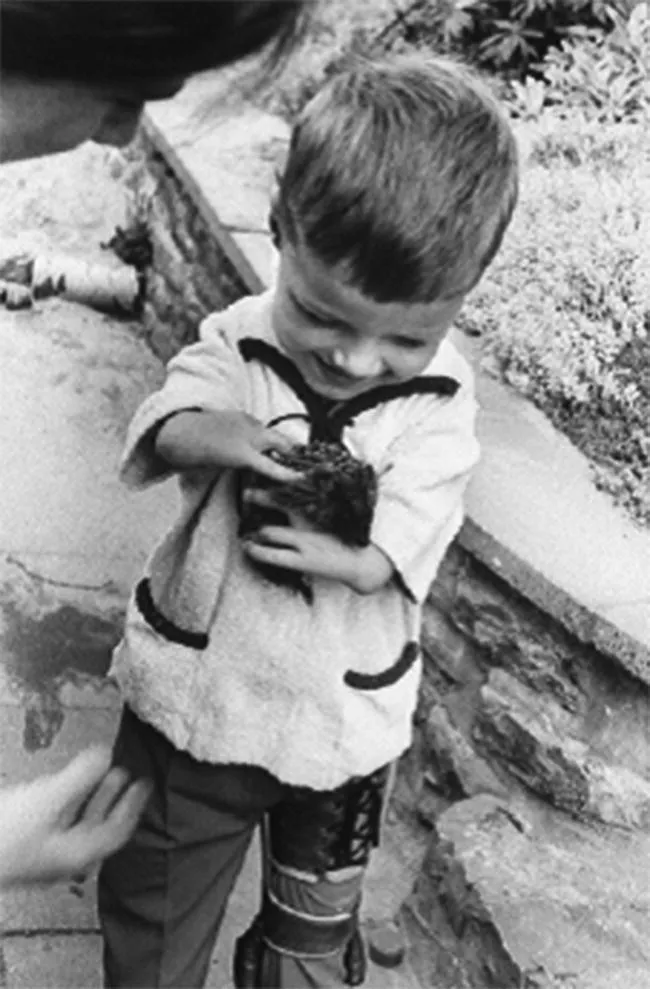
In the late 1950s there was little, if any, regulation of medicines outside the USA (where thalidomide was not allowed on to the market), and their testing and development was almost entirely in the hands of pharmaceutical companies. In the case of thalidomide, unjustified claims of safety in pregnancy were made, and its use as a sedative and treatment for nausea and vomiting was targeted at pregnant women. The drug turned out to be a teratogen, producing a variety of birth defects but particularly limb defects known as phocomelia (Figure 1.1). Worldwide, about 10 000 babies were affected, particularly in Germany where the drug was first marketed. As phocomelia was otherwise a very rare congenital abnormality, a major increase in its incidence did not go unnoticed in Germany, but the cause was initially thought to be environmental. In 1961, a series of just three cases of congenital anomalies associated with thalidomide use in Australia was reported in The Lancet, the problem was finally recognised and the drug withdrawn from sale.
Figure 1.1 Child affected by thalidomide‐induced phocomelia.
At the beginning of the 1960s, publication of possible adverse effects of drugs in the medical literature was effectively the only mechanism for drawing attention to them. Thalidomide produced a non‐lethal but visible and shocking adverse effect, leading people to ask why so many damaged babies had been born before anything had been done? This question is central to subsequent developments. It is unlikely that we will ever be able to predict and prevent all the harms that may be caused by medicines, but limiting the damage to much smaller numbers is now achievable. Today we would expect to be able to identify an association between drug and outcome analogous to thalidomide and phocomelia after the occurrence of less than 10 cases, so at least three orders of magnitude more effectively than six decades ago.
The overriding lesson learnt from thalidomide was that we cannot just wait until a drug safety problem hits us. The thalidomide tragedy of the 1960s led directly to the initial development of the systems we have in place today, although it is only since the early 1990s that the term pharmacovigilance has become widely accepted.
Pharmacovigilance is defined by the World Health Organization as ‘The science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug‐related problems.’ There are other definitions but this very broad one seems to be the most appropriate because there is a clear implication that the process is one of risk management. This is a concept that is applicable to many aspects of modern life but, surprisingly, its explicit use in relation to pharmaceuticals is a fairly recent development.
Thalidomide is not merely of historical interest, as in recent years it has made a comeback on to the market in some countries but with very narrow indications and extensive safeguards. The reasons for this exemplify the point about risk management, as the risk of fetal malformation can be successfully managed by avoidance of the drug during pregnancy. It also demonstrates another concept that is central to the practice of pharmacovigilance – the balance of benefit and risk. Thalidomide has benefits in some diseases that are otherwise difficult to treat (e.g. refractory multiple myeloma) and these appear to outweigh the risk of fetal malformation if there is an effective pregnancy prevention scheme in place. A further point that thalidomide illustrates well – and which is relevant to many other drug safety issues – is that not everyone is at the same risk of a particular adverse effect. In this case, a substantial part of the population (including men and also women who are not of childbearing capacity) are not at risk of phocomelia.
Main Lessons Learned from Thalidomide
The thalidomide tragedy taught us many lessons:
The need for adequate testing of medicines prior to marketing.
The need for government regulation of medicines.
The need for reporting systems to identify the adverse effects of medicines.
The potential safety implications of unproven marketing claims.
Most medicines cross the placenta and this results in fetal exposure.
Avoidance of unnecessary use of medicines in pregnancy.
That some risks can be successfully minimised.
The ramifications of the thalidomide tragedy were manyfold, but the key lesson for the development of pharmacovigilance was that active systems for detecting hazards are needed. Within a few years this had been taken forward with the introduction of voluntary (or ‘spontaneous’) schemes for reporting of suspected adverse drug reactions (ADRs). These have stood the test of time as an alerting mechanism or early warning system, and are covered in more detail in Chapter 3.
Scope and Purposes of Pharmacovigilance
In the past, the process of pharmacovigilance has often been considered to start when a drug is first authorised for use in ordinary practice. Nowadays, it is more commonly considered to include all safety‐related activity beyond the point at which humans are first exposed to a new medicinal product.
The ultimate purpose of pharmacovigilance is to minimise, in practice, the potential for harm that is associated with all active medicines. Although data about all types of ADRs are collected, a key focus is on identifying and preventing those that are defined to be serious. This is generally defined as an ADR that meets at least one of the following criteria:
Fatal
Life‐threatening
Causes or prolongs hospitalisation
Results in long‐term disability
All congenital anomalies.
The definition of serious also allows the application of medical judgement, such that a reaction can be considered serious even if there is not clear evidence that one of the above criteria is met. Non‐serious reactions are important to individual patients and health professionals involved in their treatment, but they can usually be managed clinically and impact less on the balance of benefit and risk for individual products and on public health in general.
Thus, pharmacovigilance can be seen as a public health function in which reductions in the occurrence of serious harms are achievable through measures that promote the safest possible use of medicinal products and/or provide specific safeguards against known hazards. Pregnancy prevention in users of thalidomide is an example of such a safeguard; monitoring white blood cell counts to detect agranulocytosis (absent white blood cells) in users of the antipsychotic drug clozapine is another (see Chapter 7).
In order to minimise harms, there is first a need to identify and assess the impact of unexpected potential hazards. For most medicines, serious ADRs are rare, otherwise their detection would result in the drug not reaching (or being withdrawn from) the market. For products that do reach the market, serious hazards are seldom identified during pre‐marketing clinical trials because sample sizes are invariably too small to detect them. In addition, the prevailing conditions of clinical trials – selected patients, short durations of treatment, close monitoring and specialist supervision – usually mean that the frequency of ADRs will be underestimated relative to what will really occur in ordinary practice.
During pre‐marketing clinical development and research on new medicines, the aims of pharmacovigilance are rather different from the broad public health functions described here. In volunteer studies and clinical trials, there is a need to protect individuals exposed to experimental products (from which they may derive no benefit) from potential harm. There is also a need to gather information on risks (including the frequencies at which they happen) in order to make a provisional assessment of safety and to plan for post‐marketing safety development (see Risk Management Planning in Chapter 5).
Development of Pharmacovigilance
We next consider some of the most important examples of drug safety issues and discuss how they have affected the development of pharmacovigilance practice from the 1960s to the present day.
Practolol
In the early 1970s another drug safety disaster occurred; this was the oculo‐mucocutaneous syndrome, a multi‐system disorder, caused by practolol (Eraldin), a cardioselective beta‐blocker used to treat angina and hypertension. As in the case of thalidomide, several thousand individuals were permanently damaged before the association was recognised. The fundamental problem in this instance was a failure of timely identification, as despite having an early warning system in place, the system was dependent on doctors suspecting an association between drug and disease. Probably because of the unusual nature of the syndrome – dry eyes, skin rash and bowel obstruction – and a long latency period (averaging almost 2 years in respect of the onset of the most serious bowel manifestations), relevant cases were not reported until the association was identified in the medical literature. Around 3000 cases were then retrospectively reported to the UK Yellow Card spontaneous ADR reporting scheme (see Chapter 3), an example of the potential effect of publicity on ADR reporting. Interestingly, subsequent attempts to develop an animal model of practolol toxicity failed, indicating that the problem could not have been predicted from pre‐clinical studies.
Main Lessons Learned from Practolol
Some adverse effects are not predictable from pre‐clinical studies.
Spontaneous reporting schemes are not always effective at identifying new ADRs.
Health professionals may not be able to identify long latency effects and clinical manifestations not known to be related to other drugs as ADRs.
Additional, proactive and more systematic methods of studying post‐marketing safety are needed.
The overriding message from practolol was that spontaneous ADR reporting alone is insufficient as a means of studying post‐marketing safety. Thus, in the late 1970s various schemes designed to closely monitor the introduction of new drugs were suggested, but few implemented. The basic idea was that initial users of new drugs would be identified through prescriptions and monitored systematically rath...
Table of contents
Cover
Title Page
Table of Contents
About the authors
Foreword
Preface to the Second Edition
Preface to the First Edition
Acknowledgements
List of Abbreviations
1 What is Pharmacovigilance and How Has it Developed?
2 Basic Concepts
3 Types and Sources of Data
4 The Process of Pharmacovigilance
5 Regulatory Aspects of Pharmacovigilance
6 International Collaboration
7 Clinical Aspects of Adverse Drug Reactions
8 Ethical and Societal Considerations
9 Future Directions
10 Learning More About Pharmacovigilance
Glossary
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access An Introduction to Pharmacovigilance by Patrick Waller,Mira Harrison-Woolrych in PDF and/or ePUB format, as well as other popular books in Medicine & Pharmacology. We have over 1.5 million books available in our catalogue for you to explore.