- Contains over 900 color illustrations, including patient photographs, chest roentgenograms, electrocardiograms, echocardiograms, angiocardiograms, 3D computed tomogramphy, magnetic resonance imaging, pathologic specimens, and other relevant visual aids
- Discusses the natural history of fetal heart disease and the rationale, indications, technique, and impact of fetal cardiac intervention
- Reviews the anatomy and physiology of the neonatal cardiovascular system, including differences within the fetal, transitional, neonatal, child and adult circulatory system
- Highlights key steps for taking a patient history, including detailed discussion of the cardiac examination (inspection, palpation and auscultation of heart sounds and murmurs)
- Presents over 35 morphologic conditions with sections covering introduction, epidemiology, etiology with accepted or postulated embryogenesis, pathophysiology, clinical presentation, physical examination findings, diagnostic evaluation, management, and prognosis
- Includes a neonatal formulary reviewing selected medications currently used for treatment of perioperative low cardiac output, congestive heart failure, pulmonary hypertension, sedation, pain and anticoagulation in neonates
eBook - ePub
Visual Guide to Neonatal Cardiology
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Visual Guide to Neonatal Cardiology
About this book
The Visual Guide to Neonatal Cardiology is a comprehensive, highly illustrated, reference covering the evaluation, diagnosis and management of cardiac disease in the newborn.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part I
Prenatal and Perinatal Issues
Chapter 1
Cardiac Embryology and Embryopathy
Robert H. Anderson1,2, Nigel A. Brown2, and Timothy J. Mohun3
1Institute of Genetic Medicine, Newcastle University, UK
2Division of Biomedical Sciences, St. George's, University of London, UK
3Developmental Biology Division, The Francis Crick Institute Mill Hill Laboratory, London, UK
As long ago as the beginning of the twentieth century, Abbott [1] argued that knowledge of embryology was essential for interpretation of congenital cardiac malformations. Only recently, however, have the necessary facts regarding the formation of the heart been sufficiently robust to underscore interpretations of the morphology of the lesions themselves. Our knowledge of cardiac development, based as it is on evidence rather than speculation, is now sufficient to help in understanding the morphology, not only of the normal heart, but also most significant congenital cardiac malformations. The advances have been made possible in no small part by the development of techniques that reveal the three-dimensional changes occurring during the processes of cardiac development [2].
Initial Stages of Development
When first recognized as having endodermal, ectodermal, and mesodermal germ layers, the developing human embryo is discoid, and the endodermal and ectodermal layers are continuous at the margins of the disc with the walls of the amnion and the yolk sac, respectively [3]. Already at this early stage, the presence of the primitive streak, with the node at its cranial end, permits recognition of the right and left sides of the developing embryo. During the subsequent stage of gastrulation, cells migrate into the mesodermal region on both sides through the primitive streak, fusing to produce the cardiac crescent. Concomitant with embryonic folding, there is folding of a trough derived from the heart-forming areas that produces the primary linear heart tube. It used to be thought that all the components of the definitive heart were present in the original tube. It is now known that, with ongoing development, new material is added to the tube at both its ends. The material of the initial tube eventually provides no more than the apex of the left ventricle (LV), and part of the muscular ventricular septum [4]. It remains moot as to whether the newly migrating cells are derived from a so-called second heart field, and whether this alleged field itself has cranial and caudal components. Suffice it to say that new cells, both myocardial and non-myocardial, continue to be added at both ends of the heart tube as it loops and separates into its right and left sides [5].
Looping of the Heart Tube
Development of the human heart is usually described using the Carnegie stages, which extend from 1 through 23, although the heart continues to show marked morphologic changes subsequent to stage 23, which is equivalent to about 8 weeks of development. The heart becomes recognizable at stage 9, equivalent to about 20 days of development. The myocardial part is then no more than a strip, anterior to paired vascular channels, with endocardial jelly interposed between the myocardial and endothelial layers [3]. By the next stage, the myocardial component has folded around the vascular elements, which are now fused to produce a tube with a solitary lumen. The connections of the lumen with the developing embryonic circulatory systems then permit recognition of the arterial and venous poles of the tube. At stage 11, representing about 25 days of development, it is possible to recognize the ventricular loop, with the atrioventricular (AV) canal positioned between the developing atrial component and the inlet of the loop. These features are seen in the developing mouse at embryonic day 9.5 (Figure 1.1). Looping is a key feature of development. The tube usually curves to the right, with the apical component of the LV then developing from the inlet part of the loop, and the apical part of the right ventricle (RV) from the outlet (Figure 1.2). The apical components of the ventricles, therefore, develop in series, unlike the atrial appendages, which develop in parallel from the atrial component of the developing heart. In the setting of visceral heterotaxy, therefore, in which there is isomerism of those features that are usually lateralized, it is only the atrial appendages that show evidence of symmetry [6]. Indeed, isomeric right atrial appendages are the prime cardiac feature of mice genetically modified by knocking out Pitx2c [7], one of the genes responsible for producing morphologic leftness (Figure 1.3). For the ventricles, however, because the apical part of each ventricle develops from a part of the tube containing both the initial right and left sides, knocking out Pitx2c does not produce evidence of ventricular isomerism. The direction of ventricular looping is random in the syndromes of visceral heterotaxy [8].
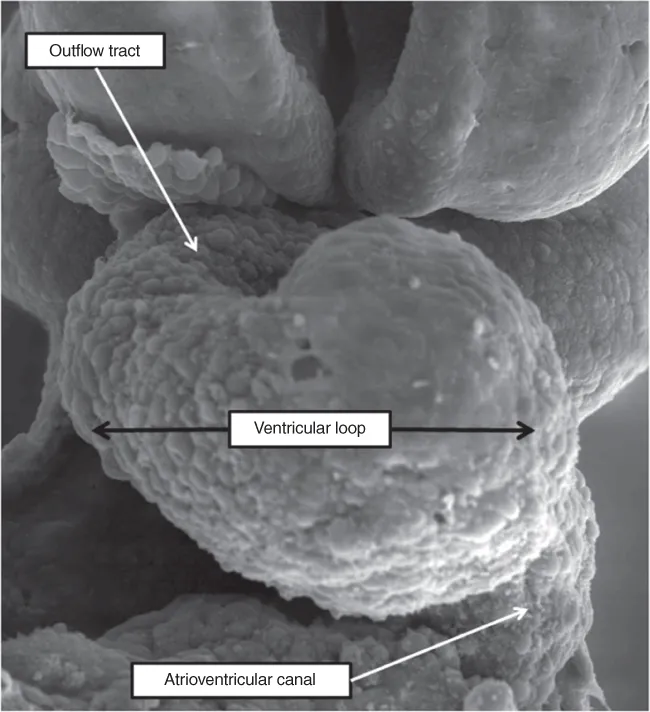
Figure 1.1 The scanning electron micrograph image shows the developing heart of the mouse at E9.5. The heart has been revealed by removing the ventral wall of the pericardial cavity. The ventricular loop extends from the atrioventricular (AV) canal, and supports the outflow tract.
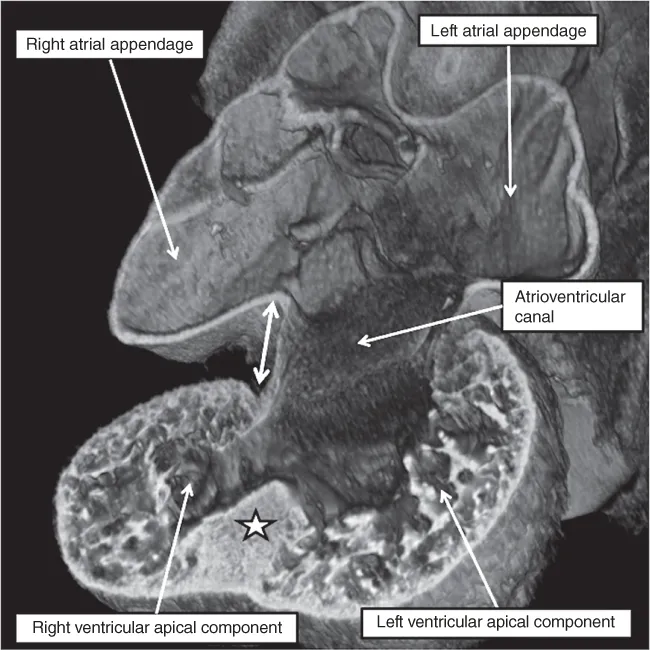
Figure 1.2 The image is prepared using an episcopic dataset from a developing mouse embryo early on embryonic day 11.5. The four-chamber section shows how the atrial appendages are beginning to balloon in parallel fashion from the common atrial chamber, while the apical components of the developing ventricles are...
Table of contents
- Cover
- Title Page
- Copyright
- Table of Contents
- Dedication
- Preface
- List of Contributors
- Part I: Prenatal and Perinatal Issues
- Part II: General Neonatal Issues
- Part III: Diagnostic Procedures
- Part IV: Specific Morphologic Conditions
- Part V: Rhythm Disturbances in the Newborn
- Part VI: Special Issues in the Newborn
- Part VII: Neonatal Formulary
- Index
- End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Visual Guide to Neonatal Cardiology by Ernerio T. Alboliras, Ziyad M. Hijazi, Cecilio (Leo) Lopez, Donald J. Hagler, Ernerio T. Alboliras,Ziyad M. Hijazi,Cecilio (Leo) Lopez,Donald J. Hagler in PDF and/or ePUB format, as well as other popular books in Médecine & Cardiologie. We have over 1.5 million books available in our catalogue for you to explore.