The market?leading at a Glance series is popular among healthcare students, and newly qualified practitioners for its concise and simple approach and excellent illustrations.
Each bite?sized chapter is covered in a double?page spread with clear, easy?to?follow diagrams, supported by succinct explanatory text.
Covering a wide range of topics, books in the at a Glance series are ideal as introductory texts for teaching, learning and revision, and are useful throughout university and beyond.
Everything you need to know about Clinical Endocrinology and Diabetes… at a Glance!
Recognizing a need to promote and enhance teaching of clinical endocrinology and diabetes in UK medical schools, the Society for Endocrinology, in collaboration with Diabetes UK and the Association of British Clinical Diabetologists, created a national curriculum that sets out the minimum recommended standards for undergraduate medical education.
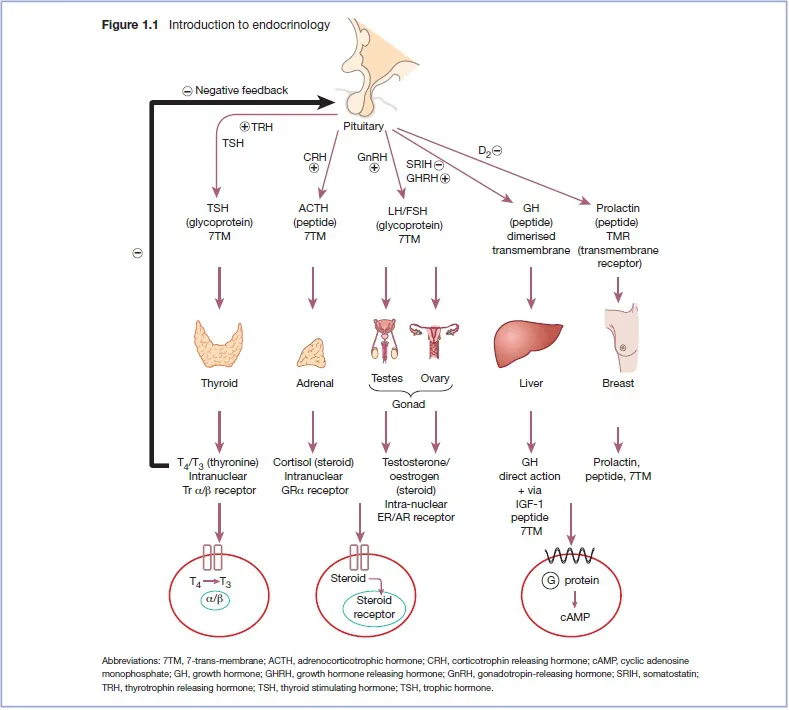
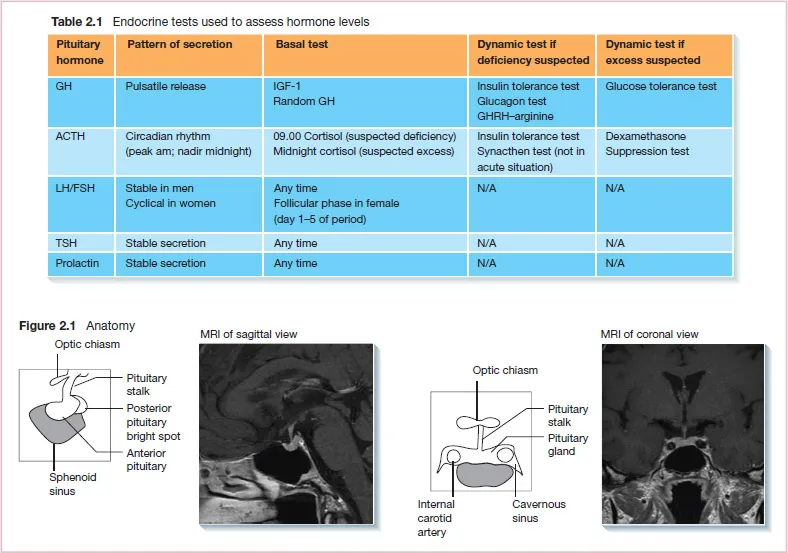
Clinical Endocrinology and Diabetes at a Glance corresponds to the curriculum and covers all important areas of diabetes and endocrinology in a clinically relevant and concise manner, with complementary figures to ensure principles are explained clearly. It highlights key practical skills for undergraduates in line with the GMC recommendations that medical graduates should be well prepared for in their Foundation posts. There is also emphasis on the importance of multidisciplinary teams in the management of endocrine diseases and diabetes. These include sections on structured education programmes, psychosocial aspects, and patient self-management and monitoring.
Clinical Endocrinology and Diabetes at a Glance will serve as a valuable resource for medical students and junior doctors treating patients with these conditions