Causes of apical periodontitis
Apical periodontitis is caused by bacterial infection of the pulp. In a healthy tooth, the pulp dentine complex is protected from oral microorganisms by the overlying enamel and cementum. However, these layers can be damaged by caries, cracks or fractures, tooth wear, restorative procedures or periodontal procedures to produce portals of entry for microorganisms.
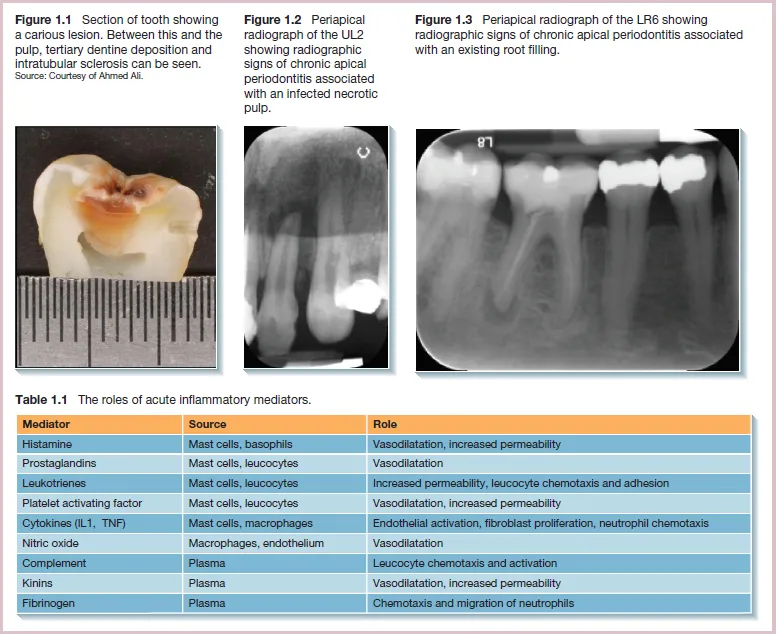
As bacteria penetrate into dentine, they release toxins that pass through the dentine tubules. The pulp responds to this by producing a layer of tertiary dentine as an additional protective layer. Increased intratubular mineral deposition may also reduce the permeability of the dentine (Figure 1.1). However, once the microorganisms penetrate into the inner dentine layers, the toxins they produce cause significant pulpal inflammation. If no treatment is provided, the bacteria eventually invade and colonise the pulp. The pulp is encased in a hard dentine shell and can therefore not expand to accommodate large amounts of fluid exudate. It also lacks sufficient collateral circulation. These factors limit the ability of the pulp to respond effectively to the insult. Pulpal inflammation can initially be reversible, with removal of the irritants resulting in resolution of the inflammation. However, as the immune challenge increases, the pulpal damage will advance beyond repair, resulting in irreversible inflammation and progressive pulpal necrosis.
Restorative procedures additionally may ‘push’ a tooth with pre-existing pulpal inflammation to irreversible pulpitis. This occurs by overheating, desiccation or chemical irritation to the dentino-pulp complex. If rubber dam is not used, or poor fitting temporary restorations are placed, microleakage can also occur. The risk of permanent damage is higher when the restorative work is close to the pulp and the dentine is permeable.
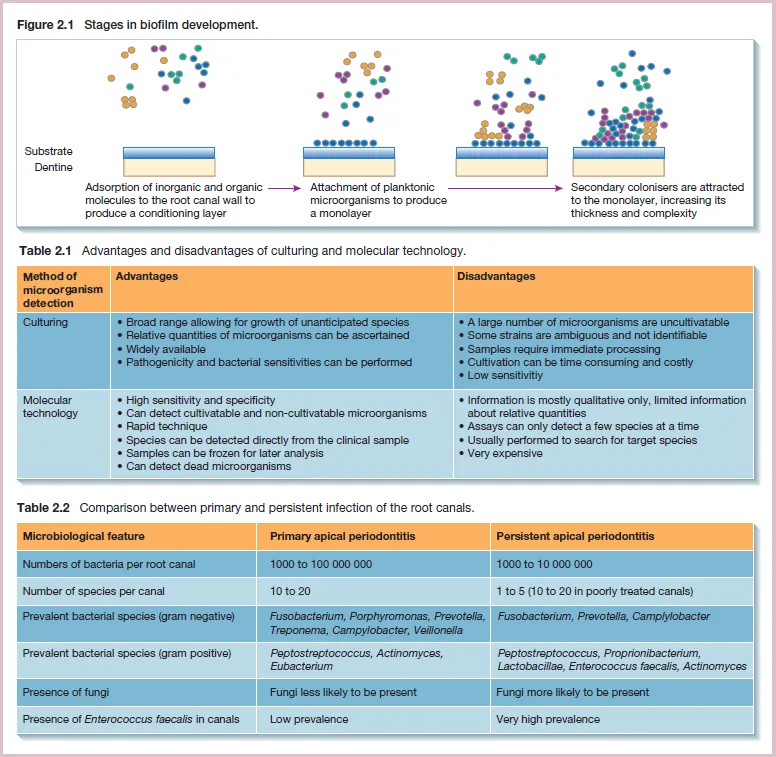
A root canal with a necrotic pulp is the ideal environment for bacterial colonisation as it provides a warm, moist, nutritious and anaerobic environment. The reduced presence of oxygen can also select aggressive anaerobic pathogens. The microorganisms are protected from the host defences as there is no blood circulation in the necrotic tissue. They derive their nutrients from the necrotic pulp tissue, periradicular tissue fluids, saliva and metabolic by-products of other bacterial species.
Over time, the bacteria progress apically down the root canal. Leakage of toxins and metabolic by-products through the apical foramen also stimulates the inflammatory response in the periapical tissues. Inflammatory mediators are released that stimulate osteoclast differentiation. This results in apical bone resorption and production of an apical lesion surrounded by chronic inflammatory cells. This stage of the disease is described as chronic apical periodontitis associated with an infected necrotic tooth (Figure 1.2).
The aim of root canal treatment is to reduce the bacterial load and seal the canals to prevent further ingress of bacteria. However, chronic inflammation can persist if inadequate disinfection is performed, with microorganisms remaining at levels sufficient to stimulate an inflammatory response. If the root canal system and coronal aspect of the tooth are not adequately sealed after root canal treatment, bacteria can re-enter and cause recurrence of the apical inflammation. It can be difficult to identify if the cause of the inflammation is persistence of, or re-entry of bacteria (or both). This stage of the disease is described as chronic apical periodontitis associated with an infected root-filled tooth (Figure 1.3).
Bacteria can egress through the apical foramen and, in some cases, cause suppuration that presents as an acute apical abscess or a chronic sinus tract.