Now in its seventh edition, this highly-regarded book is designed as an introductory and reference text on the principles of diagnosis, staging, and treatment of tumors. As for the last 6 editions of the book, the aim and scope of the new edition are once again to provide a thorough yet reasonably brief account of the whole field of oncology, focusing on the latest principles of cancer management.
The book is already well established, having been first published in 1986 and in continuous print since then. The authors are rightfully proud of their strong legacy of providing carefully revised new editions of this standard and well-received cancer text for audiences in the UK and abroad. Oncology is a very rapidly changing speciality, with many new treatments and even treatment modalities coming on stream with bewildering speed. Besides a thorough general updating of the text, figures, and tables, the new seventh edition adds a new chapter on Molecular Targeted Therapy, making the book 30 chapters in total. This accessible and practical resource is invaluable to trainees and specialists alike in oncology, palliative care and general medicine, as well as specialist nurses, general practitioners, medical students, and professions allied to medicine.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Chapter 1 The modern management of cancer: an introductory note
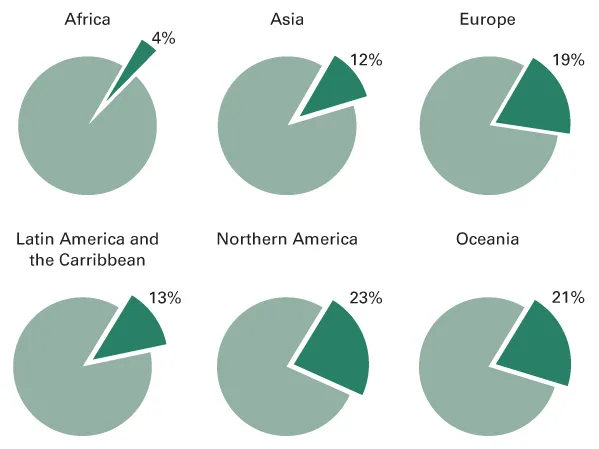
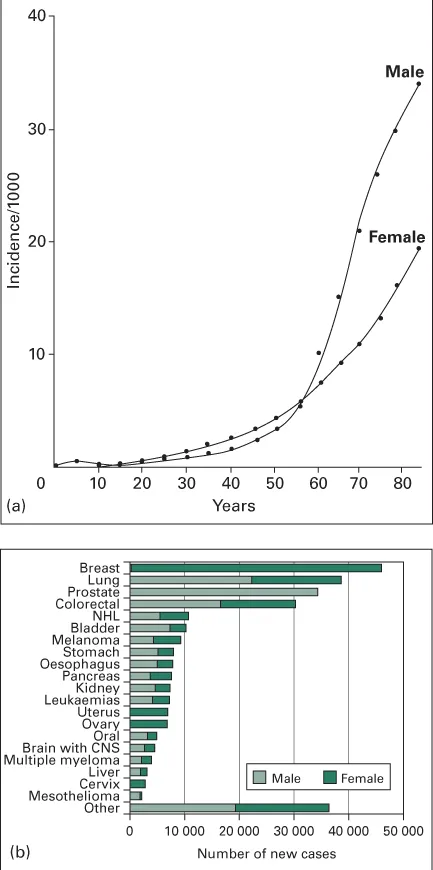
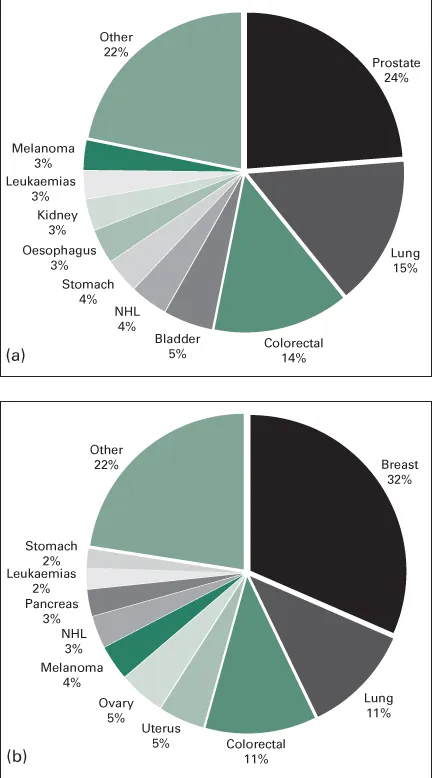
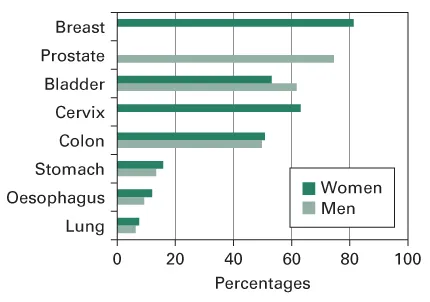
Cancer is a vast medical problem. It is now the major cause of mortality, both in the UK and elsewhere in the Western world [1] (Figure 1.1), diagnosed each year in one in every 250 men and one in every 300 women. The incidence rises steeply with age so that, over the age of 60, three in every 100 men develop the disease each year (Figure 1.2a). It is a costly disease to diagnose and investigate, and treatment is time-consuming, labour-intensive and usually requires hospital care. In the Western world the commonest cancers are of the lung, breast, skin, gut and prostate gland [2, 3] (Figures 1.2b and 1.3). The lifetime risk of developing a cancer is likely to alter sharply over the next decade because the number of cancer cases has risen by nearly one-third over the past 30 years. An ageing population, successes from screening and earlier diagnosis have all contributed to the rise. Present estimates suggest that the number of cases is still rising at a rate of almost 1.5% per annum. The percentage of the population over the age of 65 will grow from 16% in 2004 to 23% by 2030, further increasing the overall incidence [4].
For many years the main methods of treating cancer were surgery and radiotherapy. Control of the primary tumour is indeed a concern, since this is usually responsible for the patient's symptoms. There may be unpleasant symptoms due to local spread, and failure to control the disease locally leads to certain death. For many tumours, breast cancer, for example, the energies of those treating the disease have been directed towards defining the optimum methods of eradication of the primary tumour. It is perhaps not surprising that these efforts, while improving management, have not greatly improved the prognosis because the most important cause of mortality is metastatic spread. Although prompt and effective treatment of the primary cancer diminishes the likelihood of recurrence, metastases have often developed before diagnosis and treatment have begun. The prognosis is not then altered by treatment of the primary cancer, even though the presenting symptoms may be alleviated. Progress in treatment has been slow but steady. Worldwide, between 1990 and 2001, the mortality rates from all cancers fell by 17% in patients aged 30–69 years, but rose by 0.4% in those aged 70 years or older [1, 5]. This may sound impressive at first reading, but the fall was lower than the decline in mortality rates from cardiovascular disease, which decreased by 9% in the 30–69 year age group (men) and by 14% in the 70 year (or older) age group. In the UK there has been a steady fall in mortality from cancer of about 1% a year since the 1990s (Figure 1.4), but with a widening gap in the differing socioeconomic groups. As the authors forcefully state [2]: ‘Increases in cancer survival in England and Wales during the 1990s are shown to be significantly associated with a widening deprivation gap in survival’. In the USA, the number of cancer deaths has now fallen over the past 5 years, chiefly due to a decline in deaths from colorectal cancer, itself thought to be largely due to an increase in screening programmes. Interestingly, the fall in mortality has also been paralleled by a reduction in incidence rates in the USA – for men since 1990 and for women since 1991 [6]. Nonetheless, cancer continues as the leading cause of death in the USA, under the age of 85 years [3].
Figure 1.4 Cancer survival rates improved between 1999 and 2004. Available at http://www.statistics.gov.uk/cci/nugget.asp?id=861. (Reproduced under the terms of the Click-Use Licence).
Every medical speciality has its own types of cancer which are the concern of the specialist in that area. Cancer is a diagnosis to which all clinicians are alerted whatever their field and, because malignant disease is common, specialists acquire great expertise in diagnosis, often with the aid of techniques such as bronchoscopy and other forms of endoscopy. Conversely, the management of cancer once the diagnosis has been made, especially the non-surgical management, is not part of the training or interest of many specialists. This has meant that radiotherapists (‘clinical oncologists’) and medical oncologists are often asked to see patients who have had a laparotomy at which a tumour such as an ovarian cancer or a lymphoma has been found, but the abdomen then closed without the surgeon having made an attempt to stage the disease properly or, where appropriate, to remove the main mass of tumour. This poses considerable problems for the further management of the patient. More generally, lack of familiarity with the principles of cancer management, and of what treatment can achieve, may lead to inappropriate advice about outcome and a low level of recruitment into clinical trials. An understanding of the principles of investigation and treatment of cancer has become essential for every physician and surgeon if the best results for their patients are to be achieved.
During the latter part of the last century, advances in the chemotherapy and radiotherapy of uncommon tumours such as Hodgkin's disease and germ-cell tumours of the testis, together with the increasing complexity of treatment decisions in more common tumours, led to a greater awareness of the importance of a planned approach to clinical management. This applies not only for the problems in individual patients, but also in the planning of clinical trials. For each type of cancer, an understanding of which patients can be helped, or even cured, can come only by close attention to the details of disease stage and pathology. Patients in whom these details are unknown are at risk from inappropriate over-treatment or from inadequate treatment, resulting in the chance of cure being missed. Even though chemotherapy has not on the whole been of outstanding benefit to patients with diseases such as squamous lung cancer or adenocarcinoma of the pancreas, it is clearly essential that clinicians with a specialized knowledge of the risks and possible benefits of chemotherapy in these and other diseases are part of the staff of every oncology department. Knowing when not to treat is as important as knowing when to do so.
For many cancers, improvements in chemotherapy have greatly increased the complexity of management. Cancer specialists have a particular responsibility to validate the treatments they give, since the toxicity and dangers of many treatment regimens mean that the clinical indications have to be established precisely. In a few cases an imaginative step forward has dramatically improved results and the need for controlled comparison with previous treatment is scarcely necessary. Examples are the early studies leading to the introduction of combination chemotherapy in the management of advanced Hodgkin's disease, and the prevention of central nervous system relapse of leukaemia by prophylactic treatment. However, such clear-cut advances are seldom made (see, e.g. Table 1.1, which outlines the modest improvement in survival for four major types of cancer between 1998 and 2003 in England). For the most part, improvements in treatment are made slowly in a piecemeal fashion and prospective trials of treatment must be undertaken in order to validate each step in management. Modest advances are numerically nonetheless important for such co...
Table of contents
Cover
Title Page
Copyright
Dedication
Preface
Acknowledgements
Abbreviations
Chapter 1: The modern management of cancer: an introductory note
Chapter 2: Epidemiology, cure, treatment trials and screening
Chapter 3: Biology of cancer
Chapter 4: Staging of tumours
Chapter 5: Radiotherapy
Chapter 6: Systemic treatment for cancer
Chapter 7: Supportive care and symptom relief
Chapter 8: Medical problems and radiotherapy emergencies
Chapter 9: Paraneoplastic syndromes
Chapter 10: Cancer of the head and neck
Chapter 11: Brain and spinal cord
Chapter 12: Tumours of the lung and mediastinum
Chapter 13: Breast cancer
Chapter 14: Cancer of the oesophagus and stomach
Chapter 15: Cancer of the liver, biliary tract and pancreas
Chapter 16: Tumours of the small and large bowel
Chapter 17: Gynaecological cancer
Chapter 18: Genitourinary cancer
Chapter 19: Testicular cancer
Chapter 20: Thyroid and adrenal cancer
Chapter 21: Cancer from an unknown primary site
Chapter 22: Skin cancer
Chapter 23: Bone and soft-tissue sarcomas
Chapter 24: Paediatric malignancies
Chapter 25: Hodgkin's lymphoma
Chapter 26: Non-Hodgkin's lymphomas
Chapter 27: Myeloma and other paraproteinaemias
Chapter 28: Leukaemia
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Cancer and its Management by Jeffrey S. Tobias,Daniel Hochhauser in PDF and/or ePUB format, as well as other popular books in Medicine & Oncology. We have over 1.5 million books available in our catalogue for you to explore.