Winner of the Council Chair's Choice Award at the 2019 British Medical Association Awards.
Cancer Prevention and Screening offers physicians and all clinical healthcare professionals a comprehensive, useful source of the latest information on cancer screening and prevention with both a global and a multidisciplinary perspective.
Includes background information on epidemiology, cancer prevention, and cancer screening, for quick reference
Offers the latest information for clinical application of the most recent techniques in prevention and screening of all major and many lesser cancer types
Emphasises the importance of multidisciplinary teamwork in cancer screening
Highlights frequent dilemmas and difficulties encountered during cancer screening
Provides clear-cut clinical strategies for optimal patient education, communication, and compliance with cancer prevention techniques
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
CHAPTER 1 Global perspectives surrounding cancer prevention and screening
Peter David Sasieni1 and Donald Maxwell Parkin2
1 School of Cancer and Pharmaceutical Sciences, King’s College London, UK
2 Nuffield Department of Public Health, University of Oxford, UK
SUMMARY BOX
The primary approach to cancer control will always be the provision of basic treatment and care. It is inconceivable that this would not be the case because of the immediacy of caring for a sick patient. Without treatment, increased awareness, early diagnosis, and screening are pointless.
Globally, the biggest challenges and greatest successes come from tobacco control and vaccination (against hepatitis B virus and human papilloma virus).
Although not currently associated with any concerted global action, obesity and alcohol control are the next most important challenges for cancer prevention.
Cervical screening is the exemplar of a simple test with the potential to prevent the majority of a particular cancer. Even so, cervical cancer remains a major health problem in most low‐income countries.
Most other forms of cancer screening rely on early detection of invasive cancer and their widespread introduction has been restricted to countries with facilities for diagnosis and treatment.
Screening for early cancers relies on expensive technologies; attempts to use cheap and simple tests have not been successful at a national population level.
Undoubtedly, early diagnosis of cancer has a large impact on morbidity and survival (and subsequent mortality). There is evidence from developed countries that stage distribution has improved over time (more early‐stage disease with a subsequent decline in late stage at presentation). Today, stage distribution in low‐ and middle‐income countries lags behind that of high‐income countries.
Stage at diagnosis can be improved by awareness campaigns, but only when care is available, accessible, and affordable.
Principles of cancer control strategy
Noncommunicable diseases, including cancer, are a current challenge to health services, and one which will increase with the ageing of the world population and changes in lifestyles [1]. The World Health Organization (WHO) strategy is to promote National Cancer Control Programmes (NCCPs) as the most effective approach for reducing the morbidity and mortality from cancer [2]. The development of an NCCP requires adequate information in order to evaluate the nature and magnitude of the cancer burden (and the availability of health‐care infrastructure), as well as the potential impact of the various possible strategies in prevention, early diagnosis/screening, treatment, and palliative care.
Prevention of cancer has to be set within the context of prevention of other noncommunicable diseases, because they have many (but not all) risk factors in common, notably those that are lifestyle related, such as smoking, alcohol, diet, overweight/obesity, and lack of physical exercise. We do not, in this chapter, discuss biomedical approaches to prevention (medication, surgery), because globally they have no role at present.
Early diagnosis is a public and health professional awareness activity, to encourage people to recognize early signs of the cancer and to seek prompt medical attention. Screening involves encouraging asymptomatic individuals to undergo tests to detect early cancer, or precancerous states. Both early diagnosis and screening have to be set within an existing health infrastructure that provides adequate resources for the management of detected cancers (without which such programmes would be ineffective). Because of the considerable resources involved, population screening programmes should be undertaken only when the prevalence of the disease to be detected is high enough to justify the effort and costs of screening, and where resources (personnel, equipment, etc.) are sufficient to cover diagnosis, treatment, and follow‐up of those with abnormal results.
Magnitude of the problem: Proportion of cancer globally attributable to preventable causes
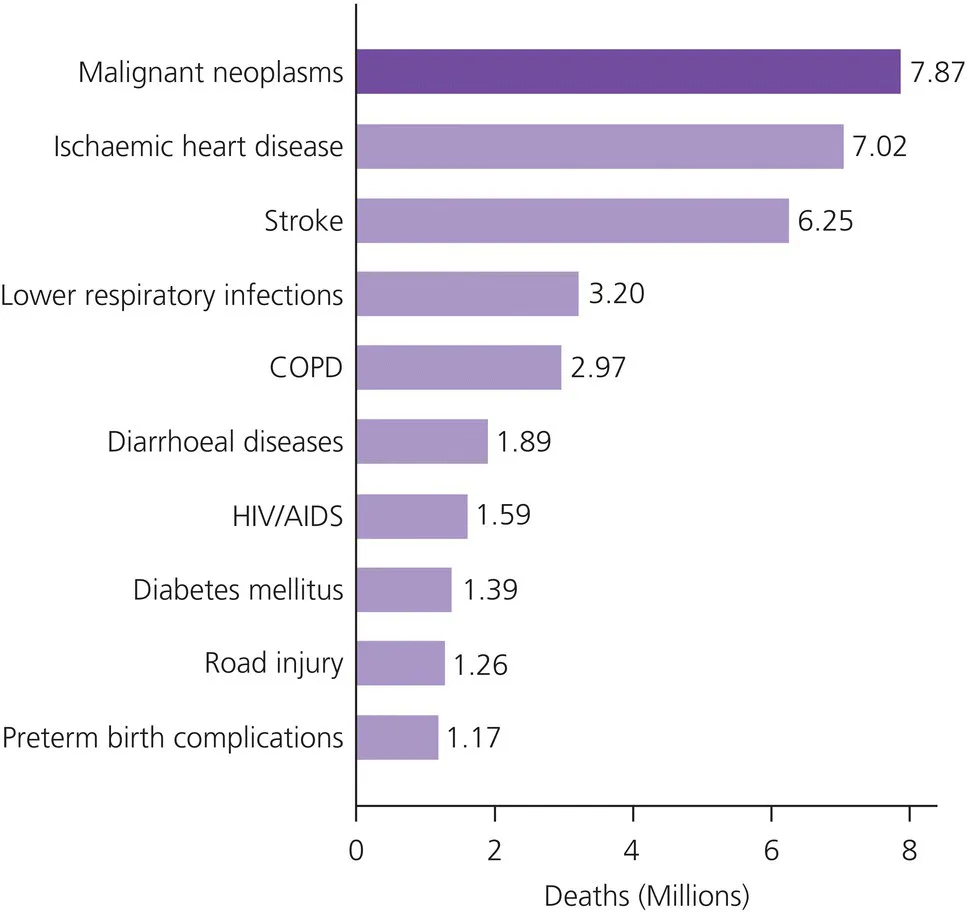
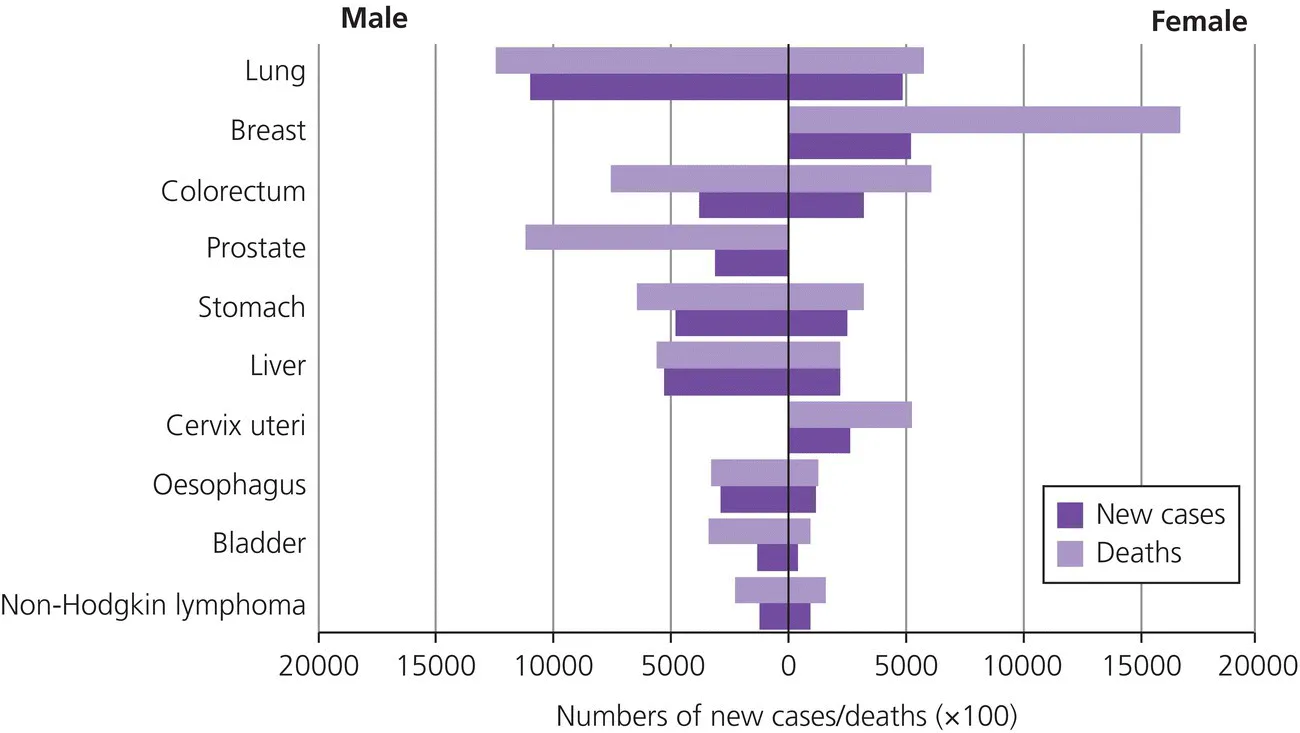
Noncommunicable diseases accounted for about two‐thirds of deaths occurring in the world in 2008 [1]. Considering cancer as a single group, the estimated 7.9 million deaths in that year constituted the leading cause of death (Figure 1.1). In 2012, the most commonly diagnosed cancers were lung cancer (13% of all cancers), breast cancer (11.9%), and colorectal cancer (9.7%); the most common causes of cancer death were lung cancer (19.4% of cancer deaths), liver cancer (9.1%), and stomach cancer (8.8%) [3]. Figure 1.2 shows the numbers of cases and deaths for the most common cancers for males and females.
Figure 1.1 The estimated 7.9 million deaths attributed to cancer in comparison to other causes of death. COPD, chronic obstructive pulmonary disease.
Source: Global Health Observatory Data Repository.
Figure 1.2 The most commonly diagnosed cancers in 2012 for males and for females.
According to Danaei et al. [4], the major environmental causes of cancer death (in 2001) were tobacco, alcohol, and low consumption of fruit and vegetables.
Tobacco smoking is undoubtedly the most important preventable cause of cancer. As estimated by the WHO [5], tobacco was responsible for 22% of the deaths from cancer in 2004 (32% in men, 22% in women), with the major contribution (58% of cancer deaths) coming from lung cancer.
Second in importance in terms of preventable causes of cancer is infection. In 2008, it was estimated that about 16% of the global cancer burden (around 2 million cancers per year) was attributable to infectious agents [6]. The fraction is much larger in low‐income than in high‐income countries. Each of the three principal infectious agents – Helicobacter pylori (stomach cancer), human papilloma virus (HPV; ano‐genital, especially cervical, and oropharyngeal cancer), and the hepatitis viruses HBV and HCV (liver cancer) – is responsible for approximately 5% of the global cancer burden. Much smaller fractions are due to Epstein‐Barr virus (nasopharynx cancers and some lymphomas) and human herpes virus 8 (Kaposi sarcoma), as well as to parasites such as Schistosoma haematobium (liver cancer) and liver flukes (cholangiocarcinoma).
The International Agency for Research on Cancer (IARC) [7] considers that there is sufficient evidence that alcohol consumption causes cancers of the oral cavity, pharynx, larynx, oesophagus, colorectum, liver (hepatocellular carcinoma), and female breast, and also that an association has been observed between alcohol consumption and cancer of the pancreas. The IARC estimated that alcohol was responsible for some 337 400 cancer deaths in 2010, 4.2% of all cancer deaths, with the largest contributions from cancers of the liver and oesophagus (about 23% of such deaths), breast, oral cavity, and colorectum (about 12% each) [7].
Approximately 2.8% of deaths worldwide are attributable to low fruit and vegetable consumption [8]; adequate consumption of fruit and vegetables reduces the risk for cancers of the oral cavity, oesophagus, stomach, and colorectum [9].
Dietary contaminants are a significant problem in some regions; for example aflatoxins, produced by moulds that contaminate cereals and nuts, cause liver cancer, especially in individuals infected with HBV. Aflatoxin has been estimated to have a causative role in 5–28% of all hepatocellular cancers [10].
In 2002, the IARC concluded that overweight and obesity are related to cancers of the colon, endometrium, kidney, and oesophagus (adenocarcinoma), as well as postmenopausal breast cancer. In addition, the report by the World Cancer Research Fund [11] considered that there was convincing evidence for an association with cancers of the pancreas and rectum, and a probable association with cancers of the gall bladder. Overweight and obesity are generally evaluated in terms of body mass index (BMI), with, in ‘western’ countries, a BMI of 25–29.9 kg/m2 being considered overweight, and over 30 kg/m2 obese. Using this definition, Renehan et al. [12] estimated that 5.7% of cancers in Europe in 2008 (3.2% of those in...
Table of contents
Cover
Table of Contents
Foreword
CHAPTER 1: Global perspectives surrounding cancer prevention and screening
CHAPTER 2: Public health perspectives surrounding cancer prevention and screening: The Ontario edition
CHAPTER 3: Cancer screening: A general perspective
CHAPTER 4: The balance of cancer screening risks and benefits
CHAPTER 5: Cancer screening issues in black and ethnic minority populations
CHAPTER 6: Public awareness of cancer screening
CHAPTER 7: Public understanding of cancer prevention
CHAPTER 8: Cervical cancer screening: An exemplar of a population screening programme, and cervical cancer prevention
CHAPTER 9: Prevention of and screening for anal cancer
CHAPTER 10: The prevention of breast cancer
CHAPTER 11: Breast cancer: Population and targeted screening
CHAPTER 12: Prostate cancer prevention
CHAPTER 13: Population screening for prostate cancer
CHAPTER 14: Colon cancer prevention
CHAPTER 15: Colon cancer screening
CHAPTER 16: Lung cancer prevention
CHAPTER 17: Lung cancer screening
CHAPTER 18: Mesothelioma: Screening in the modern age
CHAPTER 19: Skin cancer prevention and screening
CHAPTER 20: Screening and prevention of oral cancer
CHAPTER 21: Oesophageal cancer
CHAPTER 22: Hepatocellular carcinoma: Prevention and screening
CHAPTER 23: Ovarian cancer prevention and screening
CHAPTER 24: Screening for testicular cancer
CHAPTER 25: Issues in paediatric cancers
CHAPTER 26: Obesity and dietary approaches to cancer prevention
CHAPTER 27: Risk profiling for cancer prevention and screening – lessons for the future
CHAPTER 28: Cancer prevention and screening: Advances to carry forward
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Cancer Prevention and Screening by Rosalind A. Eeles, Christine D. Berg, Jeffrey S. Tobias, Rosalind A. Eeles,Christine D. Berg,Jeffrey S. Tobias in PDF and/or ePUB format, as well as other popular books in Medicine & Oncology. We have over 1.5 million books available in our catalogue for you to explore.