Written for the clinician, Cone Beam Computed Tomography helps the reader understand how CBCT machines operate, perform advanced diagnosis using CT data, have a working knowledge of CBCT-related treatment planning for specific clinical tasks, and integrate these new technologies in daily practice.
This comprehensive text lays the foundation of CBCT technologies, explains how to interpret the data, recognize main pathologies, and utilize CBCT for diagnosis, treatment planning, and execution. Dr. Sarment first addresses technology and principles, radiobiologic risks, and CBCT for head and neck anatomy. The bulk of the text discusses diagnosis of pathologies and uses of CBCT technology in maxillofacial surgical planning, orthodontic and orthognathic planning, implant surgical site preparation, CAD/CAM surgical guidance, surgical navigation, endodontics airway measurements, and periodontal disease.
eBook - ePub
Cone Beam Computed Tomography
Oral and Maxillofacial Diagnosis and Applications
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Cone Beam Computed Tomography
Oral and Maxillofacial Diagnosis and Applications
1
Technology and Principles of Cone Beam Computed Tomography
This chapter aims to convey a basic technical familiarity with compact Cone Beam Computed tomography (CBCT) systems, which have become prevalent since the late 1990s as enablers of in-office CT imaging of the head and neck. The technical level of the chapter is designed to be accessible to current or candidate end users of this technology and is organized as follows. In Section 1, a high-level overview of these systems is given, with a discussion of their basic hardware components and their emergence as an alternative to conventional, hospital CT. Section 2 gives a treatment of imaging basics, including various aspects of how a CT image is derived, manipulated, and evaluated for quality.
Section 1: Overview of compact cone beam CT systems
Computed tomography (CT) is an imaging technique in which the internal structure of a subject is deduced from the way X-rays penetrate the subject from different source positions. In the most general terms, a CT system consists of a gantry which moves an X-ray source to different positions around the subject and fires an X-ray beam of some shape through the subject, toward an array of detector cells. The detector cells measure the amount of X-ray radiation penetrating the subject along different lines of response emanating from the source. This process is called the acquisition of the X-ray measurements. Once the X-ray measurements are acquired, they are transferred to a computer where they are processed to obtain a CT image volume. This process is called image reconstruction. Once image reconstruction has been performed, the computer components of the system make the CT image volume available for display in some sort of image viewing software. The topics of image reconstruction and display will be discussed at greater length in Section 2.
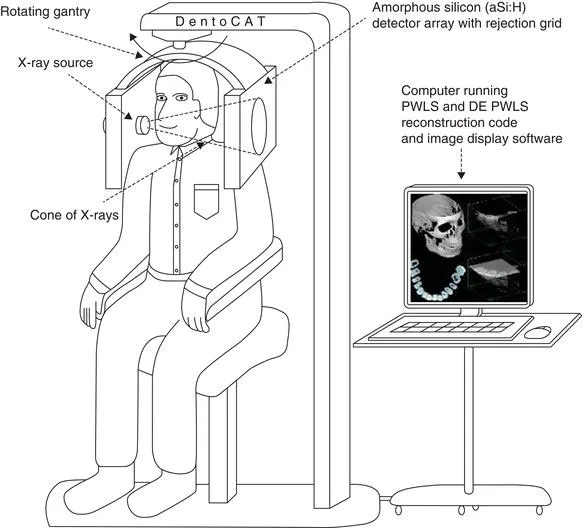
Cone beam computed tomography refers to CT systems in which the beam projected by the X-ray source is in the shape of the cone wide enough to radiate either all or a significant part of the volume of interest. The shape of the beam is controlled by the use of collimators, which block X-rays from being emitted into undesired regions of the scanner field of view. Figure 1.1 depicts a CBCT system of a compact variety suitable for use in small clinics. In the particular system shown in the figure, the gantry rotates in a circular path about the subject firing a beam of X-rays that illuminates the entire desired field of view. This results in a series of two-dimensional (2D) images of the X-ray shadow of the object that is recorded by a 2D array of detector cells. Cone beam CT systems with this particular scan geometry will be the focus of this book, but it is important to realize that in the broader medical imaging industry, CT devices can vary considerably both in the shape of the X-ray beam and the trajectory of the source.
Figure 1.1 The proposed design of DentoCAT. The patient is seated comfortably in chair (the chin-rest is not shown). DentoCAT features cone beam geometry, aSi:H detector array, PWLS and DE PWLS reconstruction methods.
Prior to the introduction of CBCT, it was common for CT systems to use so-called fan beam scan geometries in which collimators are used to focus the X-ray beam into a flat fan shape. In a fan beam geometry, the source must travel not only circularly around the subject but also axially along the subject’s length in order to cover the entire volume of interest. A helical (spiral) source trajectory is the most traditional method used to accomplish this and is common to most hospital CT scanners. The idea of fan beam geometries is that, as the source moves along the length of the subject, the X-ray fan beam is used to scan one cross-sectional slice of the subject at a time, each of which can be reconstructed individually. There are several advantages to fan beam geometries over cone beam geometries. First, since only one cross-section is being acquired at a time, only a 1-dimensional detector array is required, which lowers the size and cost of the detector. Second, because a fan beam only irradiates a small region of the object at a given time, the occurrence of scattered X-rays is reduced. In cone beam systems, conversely, there is a much larger component of scattered radiation, which has a corrupting effect on the scan (see “Common Image Artifacts” section). Finally, in a fan beam geometry, patient movement occurring during the scan will only degrade image quality in the small region of the subject being scanned when motion occurs. Conversely, in cone beam systems, where larger regions of anatomy are irradiated at a given time, patient movement can have a much more pervasive effect on image quality.
The disadvantage of fan beam geometries, however, is their inefficient use of X-ray output. Because collimators screen away X-ray output from the source except in the narrow fan region of the beam, much of the X-rays generated by the source go unused. Accordingly, the source must generate more X-ray output than a cone beam geometry for the same region scanned, leading to problems with source heating. Regulating the temperature of the source in such systems requires fast rotating source components, accompanied by a considerable increase in mechanical size, complexity, and expense. As the desire for greater volume coverage has grown in the CT industry, the difficulties with source heating have been found to outweigh the advantages of fan beam scanning, and the CT industry has been gradually moving to cone beam scan geometries. Cone beam geometries have other advantages as well, which have further motivated this shift. The spatial resolution produced by cone beam CT scanners, when used in conjunction with flat panel X-ray detectors, tends to be more uniform than fan beam–based systems.
Although the CT industry as a whole has been trending toward cone beam scanning, the hardware simplifications brought on by CBCT have played a particularly important role in the advent of compact in-office CT systems, of the kind shown in Figure 1.1. Conventional hospital CT scanners are bulky and expensive devices, not practical for in-office use. The reason for their large size is in part due to source cooling issues already mentioned and in part due to the fact that hospital CT systems need to be all-purpose, accommodating a comprehensive range of CT imaging tasks. To accommodate cardiac imaging, for example, hospital CT systems must be capable of very fast gantry rotation (on the order of one revolution per second) to deal with the movement of the heart. This has further exacerbated the mechanical power requirements, and hence the size and expense of the system.
The evolution of compact CT came in part from recognizing how cone beam scanning and other system customizations can mitigate these issues. As discussed, the use of a cone beam scanning geometry increases the efficiency of X-ray use, leading to smaller and cheaper X-ray sources that are easier to cool. Additionally, the imaging needs of dentomaxillofacial and otolaryngological medical offices have generally been restricted to high-contrast differentiation between bone and other tissues in nonmotion prone head and neck anatomy. CT systems customized for such settings can therefore operate both at lower X-ray exposure levels and at slower scanning speeds (on the order of 20–40 sec) than hospital systems. Not only does this further mitigate cooling needs of the X-ray source, it also leads to cheaper and smaller gantry control components.
The emergence of compact CBCT was also facilitated in part by recent progress in fast computer processor technology and in X-ray detector technology. The mathematical operations needed to reconstruct a CT image are computationally intensive and formerly achievable at clinically acceptable speeds only through expensive, special purpose electronics. W...
Table of contents
- Cover
- Title page
- Copyright page
- Dedication
- Contributors
- Preface
- Acknowledgments
- Oral and Maxillofacial Diagnosis and Applications
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Cone Beam Computed Tomography by David Sarment in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.