Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and Management is a modern, expertly crafted and clinically focused guide to the diagnosis, management and best-practice care of patients suffering from pancreatic cancer, cystic neoplasms and endocrine tumours.
Packed with outstanding figures and with reference to the leading society guidelines, its main focus is on the many endoscopic and radiologic diagnostic techniques, medical and surgical management of both full-blown cancer and other tumors, and the risks of each form of treatment. Also covered in detail are issues of tumor recurrence and long-term outcome of treatment.
Brought to you by highly skilled national and international leaders in the specialty and an experienced editor team, this is an invaluable guide to practicing gastroenterologists and surgeons in the hospital and clinical environment, as well as oncologists and endocrinologists managing patients with pancreatic tumorous lesions.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
CHAPTER 1 Histologic Classification and Tumor Staging of Pancreatic Cancer
Akio Yanagisawa and Eiichi Konishi
Kyoto Prefectural University of Medicine, Kyoto, Japan
Histologic Classification of Pancreatic Ductal Neoplasms
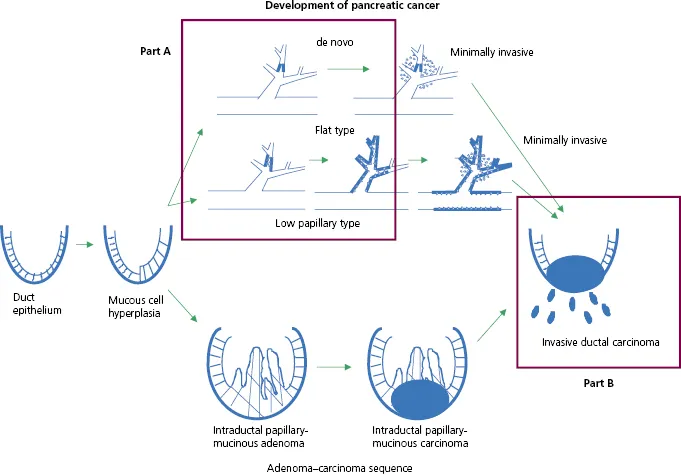
Ductal adenocarcinoma of the pancreas originates from the epithelium of the pancreatic duct and morphologically simulates it. To understand the classification of ductal adenocarcinomas of the pancreas correctly, it is important to know the basic rationale underlying the classification. Figure 1.1 shows the developmental pathway of the ductal adenocarcinoma, from ductal epithelium to invasive ductal carcinoma (1,2). The histological classification of the Japan Pancreas Society [Table 1.1 (Ref. 3)] and the World Health Organization (WHO) classification [Table 1.2 (Ref. 4)] have become widely accepted.
Figure 1.1 Developmental pathway of ductal adenocarcinoma, from ductal epithelium to invasive ductal carcinoma. Part A is classified as “carcinoma in situ” and Part B is classified as “invasive ductal carcinoma.”
Table 1.1 Histological classification and distribution of pancreatic ductal carcinoma in Japan, 2001–2007a
Number of patients
(%)
1 Atypical epithelium (AE) and carcinoma in situ (CIS)
14
(0.3)
2 Invasive ductal carcinomas (IDCs)
a Papillary adenocarcinoma (pap)
78
(1.4)
b Tubular adenocarcinoma (tub)
4564
(83.79)
i Well-differentiated type (tub1)
ii Moderately differentiated type (tub2)
c Poorly differentiated adenocarcinoma (por)
612
(11.2)
d Adenosquamous carcinoma (asc)
99
(1.8)
e Mucinous carcinoma (muc)
49
(1.0)
f Anaplastic carcinoma
37
(0.7)
i Giant cell type
ii Osteoclast-like giant cell type or giant cell carcinoma of osteoclastoid type
iii Pleomorphic type
iv Spindle-cell type
Total
5453
(100%)
a Data from Japanese Nationwide Pancreatic Cancer Registry. Courtesy of Japan Pancreas Society.
Table 1.2 WHO classification of tumors of the pancreatic ductal neoplasma
Undifferentiated carcinoma with osteoclast-like giant cells
a Data from Reference 4, Bosman et al., 2010.
According to the Japanese classification, Part A in Fig. 1.1 is classified as “carcinoma in situ” and Part B in Fig. 1.1 is classified as “invasive ductal carcinoma” and as “intraductal papillary mucinous neoplasm (IPMN), minimally invasive” or “IPMN, invasive.” Invasive ductal carcinoma is classified into six histological subtypes.
According to the WHO classification, Part A in Fig. 1.1 is classified as “pancreatic intraepithelial neoplasia (PanIN), grade 3” and Part B in Fig. 1.1 as “ductal adenocarcinoma” and “IPMN with an associated invasive carcinoma.” Ductal adenocarcinoma is also classified into six histological subtypes.
There is no significant difference between these two classification systems. This chapter discusses histological features of ductal adenocarcinoma according to the Japanese classification. IPMN is separately discussed in Section III, Chapters 27–39.
Atypical Epithelium and Carcinoma insitu
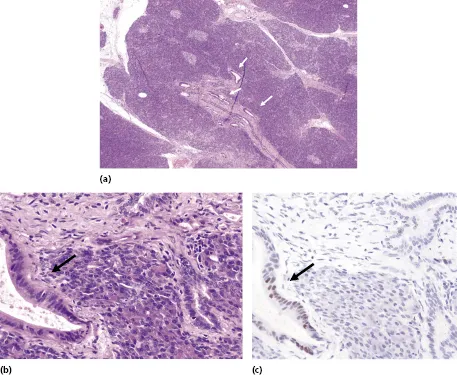
Carcinoma in situ (CIS) is a carcinoma limited to the pancreatic duct (Fig. 1.2 and Fig. 1.3a). Unlike IPMN, the duct affected with CIS is usually not dilated markedly and the dilatation is usually less than 5 mm. Histologically, it shows a completely flat or low papillary growth of atypical cells. The diagnosis of malignancy is usually based on cytologic atypia. On immunohistochemistry, p53 may be diffusely or strongly positive in the nuclei. This might be helpful in the differential diagnosis. Atypical epithelium (AE) is a lesion without as much cellular atypia as CIS.
Figure 1.2(a) Very small ductal adenocarcinoma (arrowheads), 3 mm in diameter. (b) Noninvasive ductal adenocarcinoma (left, arrow) and normal pancreatic duct (right). (c) Immunofluorescence shows the atypical duct (left, arrow) is positive for p53, but the normal pancreatic duct (right) is negative.
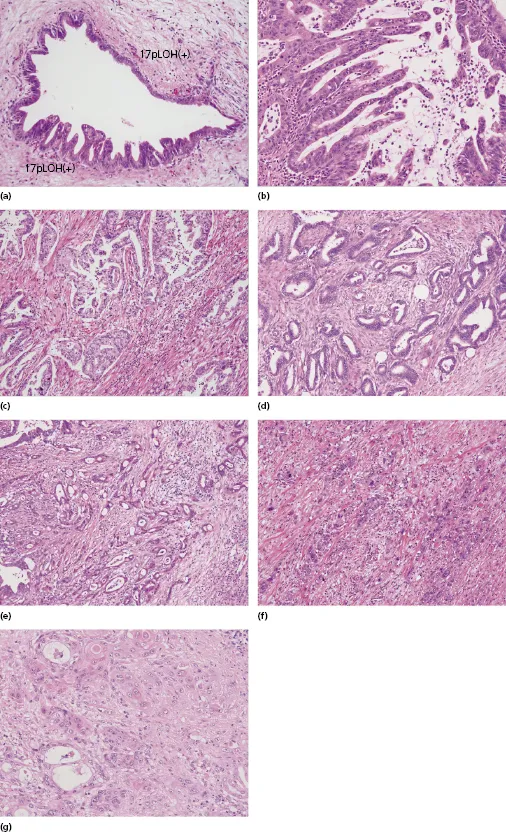
Figure 1.3 Differential variants of ductal adenocarcinoma: (a) carcinoma in situ, flat type and low papillary type; (b) papillary adenocarcinoma (pap); (c) papillotubular adenocarcinoma, well-differentiated type; (d) tubular adenocarcinoma, well-differentiated type (tub1); (e) tubular adenocarcinoma, moderately differentiated type (tub2); (f) poorly differentiated adenocarcinoma (por); (g) adenosquamous carcinoma (asc).
Invasive Ductal Carcinomas
Invasive ductal carcinomas (IDCs) are the most common neoplasm in the pancreas. According to the cancer registry of the Japan Pancreas Society (2001–2007), IDCs represent 74% of all pancreatic tumors (5449 of 7356 cases) and 82% of all pancreatic exocrine carcinomas (5449 of 6621 cases). The cut surface of an IDC is usually firm and fibrous. Medullary lesions, such as undifferentiated (anaplastic) carcinoma, are rarely present. Histologically, IDCs are subclassified into six subtypes. Tubular adenocarcinoma is the most common subtype (84% of IDCs; Table 1.1).
Papillary adenocarcinoma is an IDC with significant papillary growth pattern (0.3% of IDCs; Fig. 1.3b). This category should not include mucinous cystadenocarcinoma or adenocarcinoma arising from IPMN, with significant papillary pattern. These should be categorized as “invasive” mucinous cystadenocarcinoma or “invasive” IPMN. Tubular adenocarcinoma has two subtypes, well-differentiated type and moderately differentiated type, graded by the degree of glandular formation (Fig. 1.3c–e).
Poorly differentiated adenocarcinoma is classified separately from tubular adenocarcinoma in the Japanese classification (Fig. 1.3f). In the WHO classification (Table 1.2), however, it is classified as tubular adenocarcinoma.
Histopathological grade of differentiation, evaluated by tubular formation, has been reported as an insignificant factor for outcome. However, according to our analysis of the outcomes of the cases with radical pancreatectomy for tubular adenocarcinoma (21 cases, 2–6 cm in the greatest dimension) in Japan, the 5-year survival rate for the patients with well-differentiated tubular adenocarcinoma (27%, 5 of 15 cases) was better than that for the patients with moderately or poorly differentiated tubular adenocarcinoma (0%, 0 of 6 cases; p = 0.105). It is necessary to elucidate whether the histopathological grading affects the patient's prognosis or not.
It is not uncommon to see squamous differentiation in pancreatic carcinoma, but adenosquamous carcinoma represents 1.8% of all IDCs (99 of 5449 cases; Fig. 1.3g). Generally, it should have an area of squamous differentiation more than 25%–30% of the tumor; otherwise it should be classified as adenocarcinoma. Pure squamous cell carcinoma is extremely rare, because one can usually find an adenocarcinoma component when the tumor is examined thoroughly. Therefore, “squamous cell carcinoma” is not included in the classification. Even if one cannot find an area of adenocarcinoma by routine examination, the tumor should be d...
Table of contents
Cover
Table of Contents
Title page
Copyright page
Contributors
Preface
Abbreviations
PART I: Ductal Adenocarcinoma of the Pancreas
PART II: Periampullary Cancers
PART III: Cystic Neoplastic Lesions of the Pancreas
PART IV: Endocrine Neoplasms of the Pancreas
PART V: Chronic Pancreatitis with Inflammatory Tumor of the Pancreas
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors by Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr, Hans G. Beger,Akimasa Nakao,John P. Neoptolemos,Shu You Peng,Michael G. Sarr in PDF and/or ePUB format, as well as other popular books in Medicine & Gastroenterology & Hepatology. We have over 1.5 million books available in our catalogue for you to explore.