Esophageal Cancer and Barrett's Esophagus, 3E, focuses on these two common and key conditions that affect the esophagus, providing expert guidance to their pathogenesis, cause, prevention, diagnosis and clinical management.
Top international names in the field examine each of the many issues involved, using the very latest evidence-based research, and clear, didactic advice allows the reader to understand the best methods of diagnosis and clinical management of each condition – whether early or late stage.
Well-illustrated and fully revised to include the latest in ACG/ASG/UEGW guidelines, it is the perfect consultation tool for gastroenterologists and oncologists managing patients with cancer of the esophagus. It is also ideal for teaching residents and fellows optimum patient management, and for identifying areas requiring future research.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Section of Gastroenterology and Hepatology, Department of Medicine, Baylor College of Medicine and Houston VA HSR&D Center of Excellence, Michael E DeBakey Veterans Affairs Medical Center, Houston, TX, USA
1.1 The incidence and mortality related to esophageal cancer
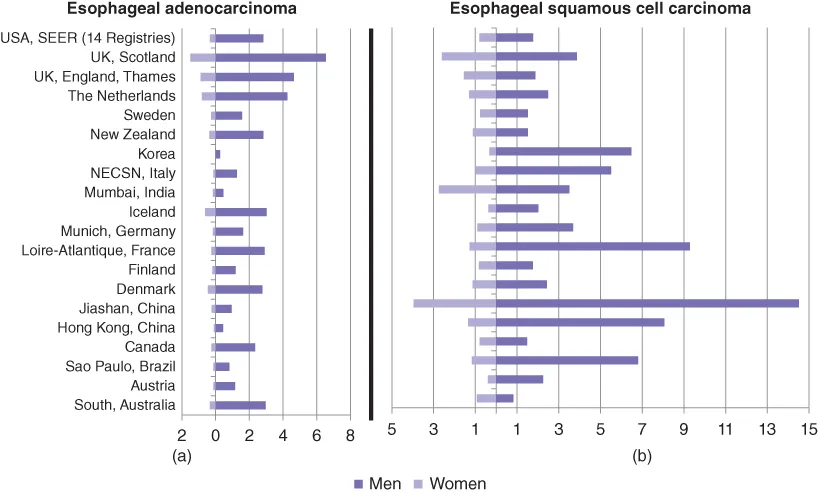
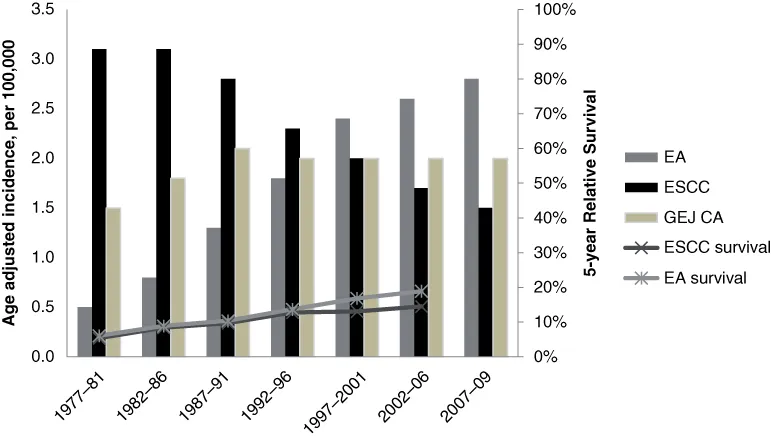
Esophageal cancer is the sixth most common cancer among men and the ninth among women, affecting more than 450,000 people globally each year. Approximately 90% of cases of esophageal cancer are squamous cell carcinoma (ESCC) [1], and the rest are adenocarcinoma (EA). The highest reported incidence and mortality rates for ESCC occur in Jiashan, China, with an age-adjusted incidence rate of 14.6 cases per 100,000 (Figure 1.1). The highest age-adjusted incidence rates of EA occur in Scotland (6.6 per 100,000) and in other parts of the United Kingdom [2]. In the United States, the age-adjusted rate of esophageal cancer in 2009 was 4.1 per 100,000; EA alone had 2.7 cancers per 100,000, a sharp increase from the 1973 rate of 0.4 cancers per 100,000 [3] (Figure 1.2)
Figure 1.1 Age-adjusted incidence rates of EA (a) and ESCC (b) in 1998-2002 using world standard population (2000). EA: Esophageal adenocarcinoma. ESCC: Esophageal squamous cell carcinoma. CI5-IX: Cancer Incidence in Five Continents, volume 9. IARC: International Agency for Research on Cancer. SEER: Surveillance, epidemiology and end results. NECSN: North East Cancer Surveillance Network.
Data from CI5-IX (2007), IARC.
Figure 1.2 Trends in incidence and five-year relative survival of EA, ESCC, GEJ-CA. Data from SEER 9 Regs research data, Nov 2011 sub, vintage 2009 pops (1973–2009) <Katrina/Rita Population adjustment> – linked to county attributes – Total US, 1969–2010 counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2012, based on the November 2011 submission. SEER: Surveillance, epidemiology, and end results. EA: Esophageal adenocarcinoma. ESCC: Esophageal squamous cell carcinoma. GEJ CA: Gastro-esophageal junction carcinoma.
Although EA is the fastest-rising malignancy among white men in the United States, its increase may be slowing [4]. The US average annual percentage change in incidence was 8.4 (95% CI 7.7–9.1) before 1997, but it decreased to 1.6 (95% CI 0.0–3.3) from 1998 to 2009 [5]. In Scandinavia, the average annual percentage change has continued to increase [6].
In addition to geographic differences in the distribution of EA, there are remarkable variations in the demographics of persons affected by this cancer. The incidence of EA increases with age and peaks in the eighth decade of life. Independent of age, however, people born in more recent years have a higher incidence of EA [7]. EA incidence is five-fold higher among non-Hispanic whites than among blacks, while ESCC incidence rates among black men are four times higher than for white men [8]. Finally, most esophageal cancer cases (77.7%) affect men [6].
The incidence of EA is 7–10 times higher in men, while the incidence of ESCC is only 2–3 times higher in men than in women, according to numerous cancer registries around the world [9, 10]. This sex discrepancy varies among different races; for example, in the 50–59 age group, the highest male-to-female ratio was 20.5 in Hispanics, followed by 10.8 in whites and then 7.0 in blacks. With EA, male predominance is evident globally (Figure 1.1). Whether the difference in incidence rates among men and women or between whites and blacks is due to less gastroesophageal reflux disease (GERD) and/or Barrett's Esophagus (BE) prevalence, or to a less progressive form of these diseases, is unknown. Despite an equal distribution of GERD between men and women [11, 12], men seem to have a more severe form of the disease, with a higher complication rate [13].
With ESCC, some areas (e.g. South Karachi, Pakistan; West Midlands, UK; Oman; Penang, Malaysia; South Australia; Kuwait) have a higher age-adjusted incidence rate among women than among men [2] (Figure 1.1). The reason behind this is unknown. The main risk factors for ESCC, which show broad regional variation, include heavy alcohol consumption, tobacco smoking and human papilloma virus infection, as well as few rare disorders, such as achalasia of the cardia, and tylosis. These will not be discussed further in this review.
1.2 Mortality
Esophageal cancer is a highly fatal disease. The overall five-year relative survival for patients diagnosed with esophageal cancer in the United States was approximately 17.3% between 2003 and 2009 (Figure 1.2). The disease stage at time of diagnosis impacts survival greatly, as the age-adjusted five-year relative survival of 38.6% in localized disease declines to 3.5% in disease associated with distant spread. However, the overall survival over the past two decades has slightly, but significantly, improved. Despite the use of screening endoscopy in high-risk groups, about 35% of EA cases between 2004 and 2010 were diagnosed at an advanced stage [14]. A higher mortality rate for nonwhite Hispanics and blacks mostly has been attributed to the decreased receipt of cancer-directed surgery, indicating possible ethnic disparities in treatment application or availability [15].
1.2.1 Progression of BE to EA
A summary of published annual EA-risk data of nondysplastic BE ranges from 0.12–0.50% to 0.33–0.70% in population-based studies and meta-analyses, respectively [16]. Recent studies have indicated that the risk of progression from BE to EA is lower than previously reported [17]. The risk in a Dutch study of 42,207 patients was 0.4% [18]; in an Irish study of 8,522 patients, it was 0.22% per year (95% CI 0.19–0.26%) [19]; and in a Danish study of 11,028 patients, it was 0.12% (95% CI 0.09–0.15) [20].
1.3 Risk factors for EA
Risk factors for esophageal adenocarcinoma are outlined in Table 1.1.
Table 1.1 Summary of risk factors for the development of esophageal adenocarcinoma
Several population-based case control studies have established a strong association, including a dose-response relationship between GERD symptoms and EA (and adenocarcinoma of the gastric cardia), but not ESCC [21, 22]. In a meta-analysis of five population-based studies, the presence of at least weekly GERD symptoms was associated with an odds ratio (OR) for developing EA of 4.92 (95% CI 3.90–6.22), which increased to 7.4 (95% CI 4.94–11.10) when the symptoms occurred on a daily basis, compared with asymptomatic controls or those with less frequent symptoms [23]. However, up to 40% of the patients with EA may not report bothersome GERD symptoms.
1.3.2 Tobacco smoking
A pooled analysis of individual data from ten case-control and two cohort studies from Australia, Canada, Ireland, the United Kingdom and the United States, including 1242 EA cases, 1263 gastroesopheageal junction cancer (GEJ-CA) cases, 954 ESCC cases and 7053 controls without cancer [24], reported an increased risk of both types of esophageal cancer with history of tobacco smoking. The calculated OR of EA increased from 1.66 (95% CI 1.1–2.4) with 1–29 pack-...
Table of contents
Cover
Title Page
Copyright
Table of Contents
List of contributors
Preface
Chapter 1: Epidemiology of esophageal carcinoma
Chapter 2: Barrett's esophagus: definition and diagnosis
Chapter 3: Epidemiology and prevalence of Barrett's esophagus
Chapter 5: Esophageal motility abnormalities in Barrett's esophagus
Chapter 6: Molecular biology of Barrett's esophagus and esophageal adenocarcinoma
Chapter 7: Histology of Barrett's esophagus: metaplasia and dysplasia
Chapter 8: Helicobacter pylori and esophageal neoplasia
Chapter 9: Screening and surveillance
Chapter 10: New surface imaging technologies for dysplasia and cancer detection
Chapter 11: New cellular imaging technologies for dysplasia and cancer detection
Chapter 12: The role of endoscopic ultrasound in esophageal cancer
Chapter 13: Staging of esophageal adenocarcinoma by CT, PET, and other modalities
Chapter 14: Medical management of Barrett's esophagus
Chapter 15: Thermal therapies and photodynamic therapy for early esophageal neoplasia
Chapter 16: RFA for early esophageal neoplasia
Chapter 17: The role of endoscopic cryotherapy for treatment and palliation
Chapter 18: Endoscopic resection
Chapter 19: Endoscopic submucosal dissection
Chapter 20: Surgical therapy of early esophageal cancer
Chapter 21: Chemoprevention: can we prevent esophageal cancer?
Chapter 22: Selection of patients for cancer prevention and eradication
Chapter 23: Combined modality therapy in locally advanced esophageal cancer
Chapter 24: Surgery in locally advanced esophageal cancer
Chapter 25: Radiation therapy for locally advanced esophageal cancer
Chapter 26: Systemic therapy and targeted agents in advanced esophageal cancer
Chapter 27: Role of endoscopy and nutritional support in advanced esophageal cancer
Index
End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Esophageal Cancer and Barrett's Esophagus by Prateek Sharma, Richard Sampliner, David Ilson, Prateek Sharma,Richard Sampliner,David Ilson in PDF and/or ePUB format, as well as other popular books in Medicine & Gastroenterology & Hepatology. We have over 1.5 million books available in our catalogue for you to explore.