![]()
1
Orthodontic Diagnosis and Treatment Planning
Normal and Ideal Occlusion
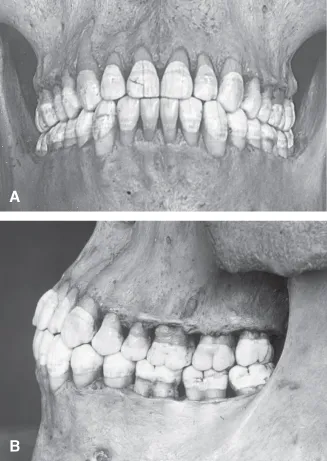
To recognize a malocclusion, a clinician needs to understand ideal and normal occlusions. People with ideal occlusions have all 32 adult teeth in superb relationships in all three planes of space. The tip of the mesiobuccal cusp of the upper first molar fits into the buccal groove of the lower first molar, and the tip of the upper canine crown fits into the embrasure between the lower canine and first premolar (Fig. 1.1, Class I ideal occlusion). Overbite, the extent that the upper central incisors overlap the lower central incisors in the vertical plane, is approximately 20%. Overjet, the distance along the anteroposterior plane between the labial surfaces of the lower central incisors and the labial surfaces of the upper central incisors, is approximately 1 to 2 mm. Teeth, moreover, are normally angled in the mesiodistal plane, normally inclined in the buccolingual plane, and aligned without being spaced, rotated, or crowded along the crests of the alveolar processes (Andrews 1972). Ideal occlusions are rare in the United States.
Normal occlusions have minimal rotations, crowding, and/or spacing of the teeth. More variability is observed in overbite and overjet in normal occlusions (Fig. 1.2). Normal occlusions are much more frequently observed in the United States than are ideal occlusions.
Normal Occlusion in the Primary Dentition
As a child approaches the age when the normal primary dentition transitions into the mixed dentition, spaces develop between the incisors in both arches with growth of the maxilla and mandible (Fig. 1.3). The spacing of primary incisors is needed to accommodate the erupting permanent incisors that are much larger than their primary counterparts.
Centric Occlusion and Centric Relation
Occlusion is observed and classified when the teeth are in maximum intercuspation, the definition for centric occlusion. Centric relation is defined as the most retruded occlusal position of the mandible from which opening and lateral movements can be performed (Moyers 1973). Centric occlusion deviated on average 0.7 mm from centric relation in 18 Class I normal occlusion subjects, with a maximum of 2.5 mm; however, in 28 Class II patients, the discrepancy averaged 1.2 mm, with a maximum of 4 mm (Williamson, Caves, Edenfield, and Morse 1978).
Angle Classification of Malocclusion
Angle classified malocclusions on the basis of the anteroposterior relationships of the upper and lower teeth (Angle 1899). He concentrated on the relationships between the upper and lower first molars and canines. His observations on the different classes remain valid and useful today. His classification system also enhances communication between clinicians.
Angle Class I Malocclusion
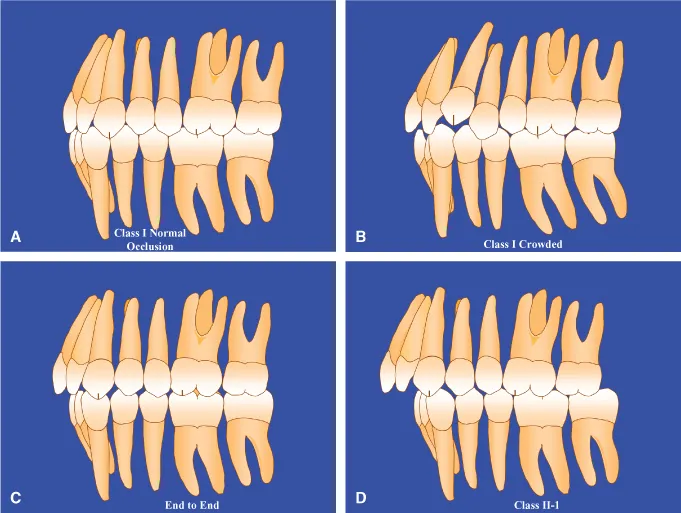
Class I malocclusions have mostly normal anteroposterior tooth relations combined with a discrepancy between tooth size and dental arch length (Fig. 1.4). The discrepancy is usually crowding and less often excessive spacing between the teeth. Patients with Class I crowded malocclusions have larger-than-normal teeth, smaller-than-normal arch lengths, and smaller-than-normal arch widths (Kuntz et al. 2008). Overbite and overjet vary in Class I malocclusions. Anterior and posterior crossbites appear in this type of malocclusion.
Class I Malocclusions in the Primary and Mixed Dentitions
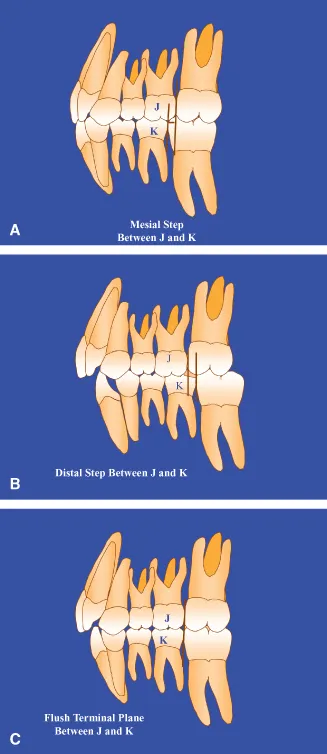
Primary second molars are considered to be Class I normal if a mesial step is present between the distal surfaces of the upper and lower molar crowns when viewed from the buccal surfaces (Fig. 1.5). A mesial step occurs when the distal surface of the lower primary second molar is mesial to the distal surface of the upper primary second molar.
Crowding problems are rarely found in the primary dentition. If no spacing is seen between the primary incisors, dental crowding can be expected. Crowding is first apparent in the mixed dentition when the permanent incisors begin to erupt. In a crowded dentition, incisors can erupt lingual and labial to the line of arch. The line of arch is located along the crest of an alveolar process where the anatomic contact points of the teeth should be located ideally on a given alveolar process. Rotated and displaced incisors are commonly seen in the developing crowded malocclusion.
Angle Class II Division 1 Malocclusion
In Class II-1 malocclusions, the lower teeth are distal to the upper teeth, usually resulting in larger-than-normal overjet. The upper incisors often have increased labial inclination, making the incisor crowns susceptible to accidental fractures. The distobuccal cusp of the upper first molar occludes with the buccal groove of the lower first molar (Fig. 1.4, Class II-1). The maxillary canine crown tip is located near the mesial surface of the mandibular canine (Fig. 1.4, Class II-1). Patients with these malocclusions may or may not have crowded arches and vary in the degree of overbite from openbite to deep overbite. On average, maxillary arch widths are narrower in Class II-1 patients than in persons with normal occlusion (Staley, Stuntz, and Peterson 1985).
Angle Class II Division 2 Malocclusion
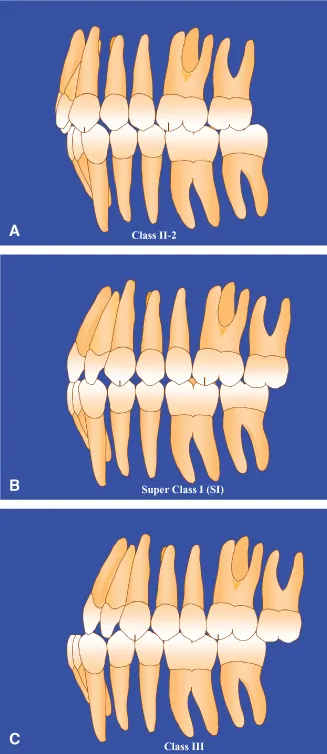
In Class II-2 malocclusions, the upper incisor crowns, especially those of the upper central incisors, are inclined to the lingual, in contrast to the excessive labial inclination observed in many Class II-1 malocclusions (Fig. 1.6). The number of maxillary incisors with lingual inclination varies from one to four. The lingual inclination of the upper central incisors results in small to moderate overjet measurements. Overbite is often deeper than normal, because of the lingual inclination of the upper incisors. The collum angle between the long axis of the crown and the long axis of the root in maxillary central incisors has been shown to be larger in a sample of Class II-2 patients compared with other occlusion groups. Class II-2 patients with large collum angles are predisposed to larger-than-normal overbites (Delivanis and Kuftinec 1980). The maxillary arches of patients with this malocclusion are narrower than normal but significantly larger than the widths observed in Class II-1 patients (Huth et al. 2007). Few of these patients have posterior crossbites.
Class II Malocclusions in the Primary and Mixed Dentitions
Primary second molar crowns are considered Class II when a distal step is observed between the distal surfaces of the upper and lower second primary molar crowns (Fig. 1.5). In this situation, the distal surface of the lower second primary molar is positioned distal to the distal surface of the upper second molar crown.
End-to-End Occlusion
When molars and canines are positioned between Class I and Class II, the relationship is considered to be end to end. These Class II malocclusions are less severe versions of the full Class II occlusion (Fig. 1.4) and are considered Class II malocclusions when assigning Angle Classification. End-to-end occlusions appear in both Class II-1 and Class II-2 types.
In the primary molars, the end-to-end relationship is expressed by what is called a flush terminal plane (Fig. 1.5). In a flush terminal plane, the distal surfaces of the upper and lower primary second molars are vertically coincident.
Angle Class III Malocclusion
In this class of malocclusion, the lower teeth are mesial to the upper teeth, usually resulting in anterior crossbite (Fig. 1.6). The mesiobuccal cusp of the upper first molar occludes with the embrasure between the lower first and second molars. Overbite varies from openbite to deep overbite. Alignment of the teeth in the arch varies from good to severe crowding, with the upper arch being more prone to crowding than the lower arch. On average, the maxillary arch widths of these patients are narrower than those in normal occlusions (Kuntz et al. 2008). The narrowness of the upper arch and the anteroposterior displacement of the arches are often associated with posterior crossbites.
Class III Malocclusions in Primary and Mixed Dentitions
Class III malocclusion in the primary dentition is expressed in an exaggerated mesial step between the distal surfaces of the upper and lower second molars. Often, in younger patients, a Class III occlusion is less severe than it will eventually become, because the mandible usually grows forward for a longer time than the maxilla.
Super Class I Malocclusions
When the mesiobuccal cusp tip of the upper first molar occludes distally to the buccal groove of the lower first molar in a position between Class I and full Class III, the malocclusion is termed Super Class I (Fig. 1.6). A Super Class I malocclusion is a mild version of Class III malocclusion and is considered a Class III malocclusion when assigning an Angle Classification to the patient.
Super Class II and Super Class III Malocclusions
These are more severe versions of Class II and Class III malocclusions and are seen only rarely. They can occur in patients who have lost teeth through extraction that permitted first molars to spontaneously move through the alveolus mesially or distally. Excessive or diminutive growth of the mandible can also result in these severe malocclusions.
Subdivision Malocclusions
Class II Subdivision Malocclusions
Class II subdivision malocclusions occur when the first molar relationship is Class II on one side of the arches and Class I on the other side. A Class II-1 subdivision is written as follows: Class II division 1 subdivision right when the Class II molar relation is on the right side of the arches and Class II-1 subdivision left when the molar relation is Class II on the left side of the arches.
The written form for Class II-2 subdivision malocclusions follows the same pattern as given earlier.
Class III Subdivision Malocclusions
Class III subdivision malocclusions occur when the first molar relationship is Class III on one side of the arches and Class I on the other side. Class III subdivision malocclusions are written as Class III subdivision right or left to indicate the Class III side.
Class II-...