![]()
Section 1
Introduction to haematology
Chapter 1 Understanding haemopoiesis
Marvelle Brown
Chapter 2 Immunology
Jane Richardson and Tracey Cutler
Chapter 3 Genes and haematology
Gwyneth Morgan
Chapter 4 The cell
Louise Knight
![]()
Chapter 1
Understanding haemopoiesis
Marvelle Brown
This chapter aims to provide an overview of the haemopoiesis process and by the end of reading this chapter you should:
- Have a detailed knowledge of all marrow cell development and function
- Be aware of the different sites of haemopoiesis
- Be aware of the role of stem cells and how they function
- Understand growth factors and how they function
Introduction
Blood is not immediately thought of as an organ, but it is one of the largest in the body. The volume of blood in adults is approximately 4.5–5 litres and marrow cells form about 40% of this volume.
Haemopoiesis is the production of marrow cells and it is a fascinating process involving a diverse range of cytokinetic interactions, which produce cells responsible for gaseous exchange, fighting infections and haemostasis. Haemopoiesis is a complex process of proliferation, differentiation and maturation, with an intricate balance between demand and supply of marrow cells. Through ongoing research of haemopoiesis and the behaviour of stem cells, their relationship with growth factors, the microenvironment of the bone marrow and regulatory mechanisms are increasing knowledge of our haematological pathologies and informing therapeutic interventions.
Haemopoiesis is the name given to the production of marrow cells and this is further subdivided into erythropoiesis (production of red blood cells), leucopoiesis (production of white blood cells) and thrombopoiesis (production of platelets). In humans there are various haemopoietic sites, starting with the blood islands in the yolk sac, which forms the basis of marrow cell production for up to two months of gestation. Red blood cells are the first to be produced, with leucopoiesis and thrombopoiesis occurring from six weeks (Pallister 1997).
During this early period the main haemoglobin being produced is Gower 1 (ζ2ε2). The liver and spleen become the main sites for marrow cell production from about two months through to seven months’ gestation and here the haemoglobin is now foetal haemoglobin, Hb F (α2γ2). From six months’ gestation the skeletal system becomes the prime source of marrow cell production and with this change in site is also a gradual change in the haemoglobin from haemoglobin F (HbF) to haemoglobin A (HbA) (α2β2). The liver and spleen continue to produce marrow cells for at least two weeks after birth, but in much reduced quantities (Hoffbrand et al. 2004). The significance of the liver and spleen being sites of early marrow cell production is significant as they can revert (back) to producing marrow cells (known as ‘extramedullary’ haemopoiesis) when the bone marrow is unable to do so or is inefficient in production due to disease, such as haemato-oncological malignancies, sickle cell disease and thalassaemia syndromes (haemoglobinopathies).
During infancy and up to three years of age the entire skeletal system produces marrow cells. Progressively, there is replacement of marrow with yellow fatty tissue in the long bones and by the early twenties the distinct skeletal sites of the vertebrae, ribs, sternum, skull, proximal end of the humerus and femur, sacrum and pelvis become the only sites for haemopoiesis. In addition, similarly to the liver and spleen, the fatty tissue in the bone marrow can also reconvert to active haemopoiesis in times of increased demand.
The bone marrow has three types of stem cells, haemopoietic stem cells responsible for the production of marrow cells, endothelial tissues, which form the sinusoids, and, finally, mesenchymal stem cells. Mesenchymal stem cells differentiate into osteoblasts (bone tissue), chondrocytes (cartilage tissue) and myocytes (muscle tissue) (Litchtman et al. 2005). The existence of stems cells other than haemopoietic stem cells found in the bone marrow has generated great interest in researchers and scientists in their potential use in treating neurological and muscular diseases in the future.
All marrow cells start their development from haemopoietic stem cells, known as multipotent or pluripotent stem cells. The terms multipotent and pluripotent refer to the fact that these cells have the ability to become any type of marrow cell. These primitive progenitor cells are unrecognisable by their cell morphology but have been identified through immunological testing as being CD34+ cells. The identification of these progenitor cells as CD34+ involves the use of a monoclonal antibody (Guo et al. 2003; Yasui et al. 2003). The term CD means cluster of differentiation and relates to what are known as surface markers on a cell which are unique to that cell.
Stems cells constitute approximately 4% of the haemopoietic cells in the bone marrow and one stem cell can produce 106 cells after 20 divisions (Hoffbrand et al. 2004). The committed progenitor cells form approximately 3% and the maturing/mature cells approximately 95% of the haemopoietic stem cells (HSC) (Traynor 2006). Stem cells also have the capacity to self-renew, which is important as this means there is always a constant supply of stem cells to respond quickly to demand such as infection, haemorrhage and anaemia. Under normal circumstances, mature marrow cells are lost through normal activities and aging.
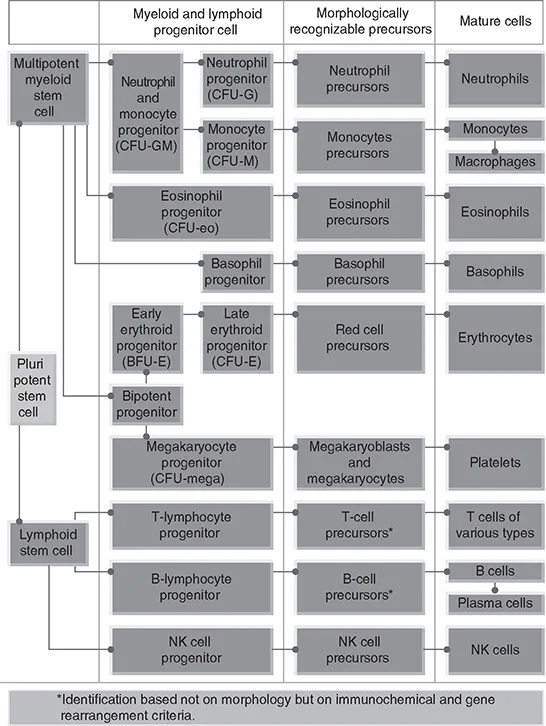
Once the HSC has been triggered all marrow cells are produced along two lines: myeloid and lymphoid. Erythrocytes, granulocytes, myelocytes and megakaryocytes are produced along the myeloid line, and lymphocytes and natural killer cells (NK) are produced along the lymphoid line. To start the differentiation process, the pluripotent stem cells can differentiate into either the precursor, colony-forming unit – granulocyte, erythrocytes, myelocytes, megakaryocytes (CFU-GEMM), or lymphoid stem cell. Differentiation of these lines produces committed cell lines. The exception is the progenitor cell, CFU-GM, which gives rise to monocytes and neutrophils. As a cell goes through its stages of development, it progressively loses its capacity to self-renew and once matured is unable to do so at all (terminal differentiation) (see Figure 1.1).
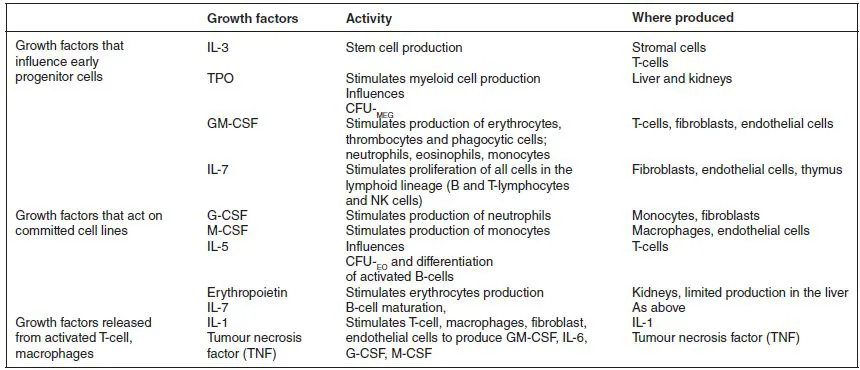
Growth factors are naturally occurring glycoproteins and determine the behaviour of the stem cell. They are produced from a number of sources: macrophages, fibroblasts, endothelial cells, monocytes, T-cells, the kidneys and the liver (Pallister 2005). Growth factors can work solely on a committed line such as erythropoietin. Others are synergistic, whilst others can influence both early progenitor cells and later committed cells. Granulocyte colony stimulating factor (G-CSF) and thrombopoietin (TPO) enhance the activities of stem cell factor (SCF), interleukin-3 (IL-3), granulocyte monocyte-colony stimulating factor (GM-CSF). In addition, G-CSF and GM-CSF enhance the function of mature cells (Hoffbrand et al. 2004; Metcalf and Nicola 1995). Our understanding of the activities of growth factors has aided in the pharmacological production of erythropoietin used in renal disease and recombinant granulocyte stimulating factor, (rHG-CSF), used in stem cell transplantation to reduce the period of neutropenia. Table 1.1 provides an overview of growth factors, their sources and functions.
The microenvironment of the bone marrow is known as bone marrow stroma and is a unique environment which forms the structural base, allowing stem cells to grow and develop. The stroma is made up of a structural base of cells which are macrophages, reticular connective tissue, osteoclasts, osteoblasts, adipocytes, fibroblasts and...