I hear so many variations of this story from patients that I have seen with sleep disturbances. I listen, and I always give the same answer: “Yes, there are significant differences between men and women, even in the very neglected area that we call sleep.”
Gender differences between men and women regarding sleep are primarily recognizable after puberty. They are a combination of many factors, including:
•The effect of hormones related to fertility in a woman’s life cycle.
•Differences in male and female sleep structures.
•Multiplicity of roles in women’s lives which affect stress and sleep levels.
•Tendency to depression and anxiety, which is twice as common in women as in men.
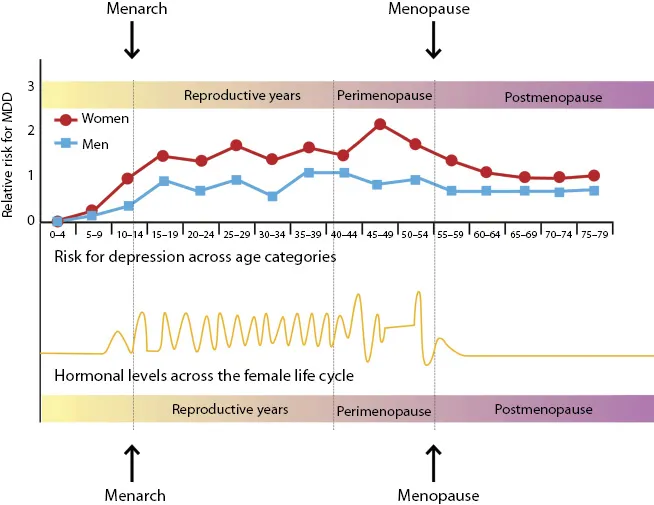
•Women’s physical and mental diseases affecting sleep (Figure 1.1).
Figure 1.1 Risk for depression across age categories.
My field of expertise as a psychiatrist is reproductive psychiatry, and it deals with the connection between hormonal and mental changes in the course of a woman’s life—that is, mental changes during the menstrual cycle, pregnancy, postpartum, and menopause. I was introduced to this field combining gynecology and psychiatry, which was new in psychiatry at the time, during a 2-year fellowship program in New York, and it fascinated me. I felt I had found my place and calling after many years of uncertainty about my chosen profession.
At a stand of professional books at a conference I attended in the United States, the book Depression in Women (2001) by psychiatrists Meir Steiner and Kimberly Yonkers, which deals with the relationship between hormonal and mental changes caught my eye. The book addresses all the stages in the life of a woman, from puberty to menopause. It touches on both normative and non-normative mental changes and explains their causes and ways of treatment. I purchased the book, and after reading it, I decided to write a similar book in Hebrew.
My book, Women, Mood and Hormones, published in 2005, was based on the experience I gained working as a psychiatrist in hospital gynecological wards in Israel. It describes the mental vicissitudes experienced by women throughout their lives: during the menstrual cycle, pregnancy, postpartum, and menopause. It addresses normative changes that do not require treatment, as well as less normative changes that cause emotional and functional disturbances and need to be treated. The book offers guidelines for treatment ranging from psychological therapy and medication to nutritional changes and alternative remedies.
The book was intended for physicians who specialize in women’s health. Surprisingly, it attracted a female readership that included women of all ages, professions, and educational and cultural backgrounds; women who were thirsty for the knowledge I presented and curious about the links between the hormonal changes they experienced and their state of mind. I resolved that my next book should also address those in need of this information—women themselves.
In the following years, a new area within my field of expertise came into focus—sleep disturbances in women. The more knowledge I gained about the subject through treating afflicted women, the more aware I became of how little this common disturbance is understood and, consequently, of the limited scope of viable solutions. I knew this would be the subject of my next book.
While working on the book, I told people close to me about its subject. Their reactions, as expected, were varied. Some wondered if there really is a difference between female and male sleep. Others thought it was an excellent idea, considering that so little is known about sleep. Almost every woman who heard about the content of the book told me that she, or a friend or relative, suffered from sleep disturbances. Everyone agreed on one thing: It is an important subject and very timely for a period in which women are asserting their place in the world and letting their voices be heard.
When I began to collect information and data, I found very little professional literature on sleep disturbances in women. Most of the existing material is in English, highly professional, and aimed at physicians, but not easily accessible for women. Indeed, it is not easy to simplify professional knowledge into a readily comprehensible language, yet that is the challenge I took upon myself.
In my role as a psychiatrist specializing in women’s health, I encountered women of various ages and circumstances, who told me of their distress concerning sleep disturbances, whether or not related to hormonal changes. Psychiatry treats sleep disturbances as part of depression or anxiety, but does not pay attention to gender differences, or take into consideration the hormonal changes that affect sleep.
The more my help was sought by women who suffered from sleep disturbances, the more intrigued I became by its causes and by methods of easing them. It is well-known that women are more likely than men to seek medical help, especially in my profession as a psychiatrist of women’s health. Yet, there is no doubt (and this is supported by the professional literature) that sleep disturbances are more common in women than men, especially in the current era in which women fill diverse roles in their lives and have an ever-decreasing number of hours of sleep.
Is the medical world dedicating resources to study and treat sleep disturbances in women in light of the above? By no means! Even today, sleep disturbances are not taught in medical schools, except in relation to other disturbances.
Clinical trials, and subsequently diagnoses and treatments, have focused on male subjects, since hormonal changes in women introduce unwanted complexity. The general assumption was that what worked for men would also work for women. We now understand that this is not the case, and we are witnessing the development of gender-specific medicine.
The first time that the U.S. Food and Drug Administration (FDA) addressed gender differences in relation to medicine dosage was in 2013. According to a statement published in medical journals, women were to be given half the recommended dose of pills containing zolpidem (Ambien, Zodorm, Stilnox). In women, these pills can impair morning alertness, cause uneasiness, and at times enhance daytime anxiety. This is only one instance of many gender-oriented differences found in the medical treatment prescribed to men and women. Most have yet to be studied and published. The FDA statement was undoubtedly a milestone in gender medicine and marked the beginning of a new era.
Women tend not to share their sleep problems with those around them. They treat it as a sentence they must accept or, at most, combat with sleeping pills.
Women of Irit’s mother’s generation tended not to talk and not to complain, and the means to help them were more limited. I explained to Irit that today there is no reason to suffer, and that menopause is one of the most common causes of sleep disturbances in women, with or without hot flashes. Irit wanted to know why the problem can’t simply be solved with sleeping pills. The answer to this is complicated, and therefore I will dedicate an entire chapter to the medical treatment of sleep disturbances.
My need to write about sleep disturbances in women came from my experience in this area as part of my job, but primarily from the distress I encountered in women close to me and in my patients. I want to encourage women to understand that it is not a sentence they have to accept. Accurate diagnosis of the sources of sleep disturbances can lead to a custom-made treatment for each woman and provide her with the help that will improve the quality of her sleep.