
Musculoskeletal MRI
Asif Saifuddin, Philippa Tyler, Rikin Hargunani
- 1,266 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
Musculoskeletal MRI
Asif Saifuddin, Philippa Tyler, Rikin Hargunani
Über dieses Buch
Musculoskeletal MRI covers the entire musculoskeletal system and related conditions, both common and rare. The text is neatly divided into sections based on the major anatomic divisions. Each section discusses anatomic subdivisions or joints, keeping sections on normal anatomy and pathologic findings close to each other, allowing radiologists to easily compare images of normal and pathologic findings.
With more than 4000 high-quality MR images, information is presented in an easy-to-read bulleted format, providing the radiologist with all the information required to make an informed diagnosis in the clinical setting. The new edition also includes a complimentary eBook as well as access to image downloads. Comprehensive and user-friendly in its approach, the book provides every radiologist, both consultant and trainee, with increased confidence in their reporting.
Häufig gestellte Fragen
Information
The Shoulder Girdle
Technique
Conventional MRI1–3
- positioning: the patient lies supine with the arm adducted and in neutral or in comfortable external rotation:
- internal rotation of the shoulder should be avoided as laterally, the tendons curve out of plane and are subject to partial volume averaging, resulting in reduced accuracy for diagnosing rotator cuff tears4
- a dedicated shoulder coil is required for high resolution imaging
- sequences:
- coronal oblique T1W/PDW FSE sequence: obtained from an axial scout and planned parallel to the supraspinatus tendon (Fig. 1.1), covering subscapularis anteriorly to infraspinatus posteriorly Fig. 1.1
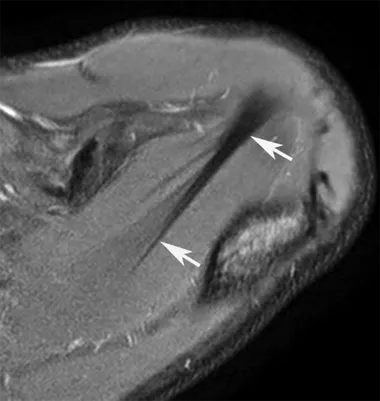 Axial FS PDW FSE MR image showing orientation of ofthe supraspinatus tendon (arrows) for planning coronal oblique MR of the shoulder.
Axial FS PDW FSE MR image showing orientation of ofthe supraspinatus tendon (arrows) for planning coronal oblique MR of the shoulder. - coronal oblique FS PDW FSE/T2W FSE sequence aligned to the supraspinatus tendon:
- the addition of FS improves diagnosis of full- and partial-thickness rotator cuff tears compared to conventional T2W FSE images
- similar information may be obtained by use of a modified STIR sequence5
- sagittal oblique T2W FSE sequence (+/-FS) obtained from an axial scout and planned perpendicular to the supraspinatus tendon, covering from the scapular neck medially to the deltoid muscle laterally
- axial T2W GRE and/or PDW FSE (+/-FS) sequence: covering from the acromion to the inferior glenoid rim
- coronal oblique T1W/PDW FSE sequence: obtained from an axial scout and planned parallel to the supraspinatus tendon (Fig. 1.1), covering subscapularis anteriorly to infraspinatus posteriorly
- post-operative shoulder:6 surgical clips/sutures may produce artefact and therefore, GRE/FS techniques are avoided and FSE and STIR are used
3T Imaging7,8
- MR imaging at 3-Tesla (3T): offers increased signal-to-noise ratio (SNR) and the potential to increase diagnostic accuracy
- a dedicated phased-array shoulder coil is used
- technical parameters at 3T: field of view (FOV) 14–16 cm, slice thickness 2–3 mm and 320 × 320 matrix
Additional Sequences
- ABER (abduction external rotation) view:9 the shoulder is positioned with the palm behind the head, usually combined with MR arthrography (Fig. 1.2) giving the advantage of: Fig. 1.2
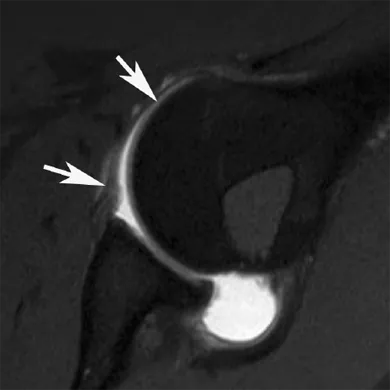 FS T1W SE direct MR arthrogram image in the ABER position showing the anterior band of the IGHL (arrows).
FS T1W SE direct MR arthrogram image in the ABER position showing the anterior band of the IGHL (arrows).- optimal demonstration of the anterior band of the inferior glenohumeral ligament (IGHL), which is placed under tension
- a statistically significant increase in sensitivity for Perthes lesions of the glenoid labrum compared with MR arthrography in the neutral position10
- detection of a posterosuperior labral peel back lesion, an injury described in the overhead throwing athlete, with a reported sensitivity of 73% and specificity of 100%11
- reported increased sensitivity for detection of partial articular-side tears of the supraspinatus tendon12
- reported improved diagnostic accuracy in anterior and posterior soft-tissue labral tears13
- ADIR (adduction internal rotation) view: performed by placing the palm behind the back:
- aids in identification of certain anterior labral abnormalities,14 including Bankart lesions in first time shoulder dislocation due to displacement of the labrum in internal rotation15
- FADIR (flexion adduction internal rotation) view: performed by placing the arm across the chest with the hand on the contralateral shoulder and the palm facing outwards:
- may increase diagnostic confidence in characterising postero-inferior labral abnormalities16
- 3D volumetric imaging:8,17,18
- has the advantage of acquiring thin continuous slices through the joint, reducing the effect of partial volume averaging
- isotropic resolution allows multi-planar reconstruction after single image acquisition, potentially eliminating the need to acquire the same sequence in different planes
- long acquisition and post-processing times have been prohibitive for incorporation into routine clinical practice: recent technical advances, including higher field MR systems, high-resolution dedicated multichannel coils, and pulse sequences with shorter acquisition times have made 3D imaging more feasible
- to date, has found greatest clinical use in the evaluation of articular cartilage
- may also improve confidence in assessing small curved structures, such as the proximal biceps tendon and curved portions of the labrum19
- reported to show similar accuracy to conventional imaging in assessing rotator cuff and labral tears, with potentially faster imaging time20,21
- 3D MR arthrography may be a promising substitute to computed tomography (CT) as a method for assessing bony Bankart lesions and glenoid bone loss22
Indirect MR Arthrography2
- involves the intravenous injection of gadolinium (at a concentration of 0.1 mmol/kg) followed by 10–15 minutes of shoulder exercise, resulting in enhancement of areas of synovitis or hypervascular repair tissue, and following diffusion of contrast into the joint space over time, produces a hyperintense joint effusion:
- the arthrographic effect is reliant upon the permeability of the synovial membrane, which may be increased in inflammatory conditions such as arthritis or infection, as well as by prior surgery23
- coronal oblique, sagittal oblique and axial FS T1W SE sequences are performed, together with a coronal oblique FS T2W FSE /STIR sequence
- indirect MR arthrography is reported to show high accuracy and sensitivity in the detection of labral abnormalities at 1.5T24
- the major disadvantage is the lack of joint distension
- other factors that can lead to suboptimal indirect arthrographic imaging include synovial fibrosis, premature scanning time or extravasation25
Direct Saline MR Arthrography26,27
- involves intra-articular injection of 12–15 ml saline under fluoroscopic control, following confirmation of intra-articular position by initial injection of 1–2 ml iodinated contrast medium
- coronal oblique, sagittal oblique and axial imaging with FS T2W FSE sequences are performed
- advantages: potential cost saving by eliminating gadolinium, improved allergy safety, and allows for a reduction in imaging time as FS T1W sequences need not be performed
- disadvantages: does not differentiate between native and injected joint fluid since both appear hyperintense:
- image resolution may be relatively poor compared to FS T1W SE images as used in direct gadolinium MR arthrography
Direct Gadolinium MR Arthrography2,28
- involves intra-articular injection of 12–15 ml dilute gadolinium/saline mixture (at a concentration of 1–2 mmol/l29) to distend the joint capsule and outline the intra-articular structures
- reported to be safe in the short term and is reasonably well tolerated:30
- the addition of local anaesthetic to the injection may reduce periprocedural pain and major motion artefacts;31 however, this beneficial effect has not been observed in all studies32
- indications include: shoulder instability, evaluation of the labrocapsular complex, rotator cuff and post-surgery
- injection is performed under fluoroscopic control using an anterior, rotator interval (RI) or posterior approach, or with ultrasound guidance for which a posterior approach appears to be preferential:33
- the anterior approach may result in damage to, or inadvertent extravasation of contrast material within, the subscapularis muscle/tendon (Fig. 1.3a), the subdeltoid bursa (Fig. 1.3b), the IGHL or the anterior glenoid labrum Fig. 1.3
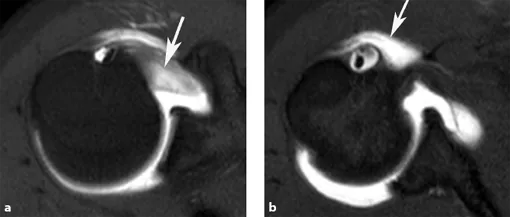 Axial FS T1W SE direct MR arthrogram images following anterior injection showing extravasation of contrast into (a) the subscapularis tendon (arrow), (b) the a b subdeltoid bursa (arrow).
Axial FS T1W SE direct MR arthrogram images following anterior injection showing extravasation of contrast into (a) the subscapularis tendon (arrow), (b) the a b subdeltoid bursa (arrow). - the RI approach is reported to result in a lower probability of injury to key intra-articular structures34
- the posterior approach does not involve the needle traversing any anterior labrocapsular structures, and may be preferential for the assessment...
- the anterior approach may result in damage to, or inadvertent extravasation of contrast material within, the subscapularis muscle/tendon (Fig. 1.3a), the subdeltoid bursa (Fig. 1.3b), the IGHL or the anterior glenoid labrum