![]()
Chapter 1
Definitions and Classification of Autism Spectrum Disorders
Melissa P. Maye, Ivy Giserman Kiss, and Alice S. Carter
Autism Spectrum Disorder, a new diagnosis in the fifth edition of the Diagnostic and Statistical Manual (DSM-5), was developed to classify individuals with impairments due to difficulties with social communication and social interaction, as well as the presence of restrictive and repetitive behaviors, interests, or activities (American Psychiatric Association, 2013). Autism Spectrum Disorder (ASD) replaces a set of diagnoses that were included in the fourth edition of the Diagnostic and Statistical Manual (DSM-IV), including Autistic Disorder, Pervasive Developmental Disorder (PDD) – Not Otherwise Specified, and Asperger’s Disorder (APA, 2000). These diagnoses were previously grouped together within a category labeled Pervasive Developmental Disorders. At present, it is estimated that one in 68 children (one in 42 boys; one in 189 girls) have an ASD diagnosis (Center for Disease Control, 2014).
In this chapter, the ways in which the conceptualization of the construct autism has changed over the last century are explored, and modifications made to the diagnostic criteria in each edition of the DSM are described. Special emphasis is placed on the most recent changes introduced in the DSM-5 in 2013. Symptom criteria that are used to diagnose Autism Spectrum Disorder in the DSM-5 are described in detail.
A number of screening tools and diagnostic measures have been developed to aid clinicians and researchers in making earlier and more accurate diagnoses of the previous diagnosis of PDD and the current diagnosis of ASD (e.g., Lord et al., 2012; Lord, Rutter, & Le Couteur et al., 1994; Luyster et al., 2009; Robins et al., 2014; Rutter, Bailey, Lord, Cianchetti, & Fancello, 2007; Schopler, Van Bourgondien, Wellman, & Love, 2010; Stone, Coonrod, & Turner; 2004; Stone, McMahon, & Henderson, 2008). In addition to reviewing historical shifts in diagnostic criteria and conceptualizations, this chapter presents three diagnostic measures that are widely used in diagnostic assessment and have strong evidentiary bases. It is important to note that while these diagnostic measures are extremely useful as aids in clinical decision-making, they are not considered diagnostic instruments. They should be used to inform, rather than to replace, clinical judgment.
Historical Changes in Diagnosis and DSM Criteria
The conceptualization of ASD has changed over time to accommodate our evolving understanding of the disorder. In 1911, Eugen Bleuler, a Swiss psychiatrist, coined the terms autism and autistic, which were developed from the root Greek word autos, meaning self. Bleuler used the term autism to describe a symptom of Schizophrenia, in which individuals actively withdrew from the external world and into themselves, “rejecting reality” (Moskowitz & Heim, 2011). Regarding this autistic behavioral pattern, Bleuler (1951) wrote, “the most severe cases withdraw completely and live in a dream world; the milder cases withdraw to a lesser degree” (p. 399). Rather than referring to individuals now understood to have ASD, Bleuler intended for his term autism to refer to the “isolated self” observed in individuals with psychosis. Thus, in DSM-I, published in 1952, the term autism was used to describe psychotic reactions observed in children with childhood-onset Schizophrenia (American Psychiatric Association, 1952). DSM-II (American Psychiatric Association, 1968) also mentioned autism only within the context of childhood Schizophrenia.
Between the 1940s and 1960s, the symptom of autism continued to be widely regarded as an early indicator of childhood Schizophrenia (Baker, 2013). Moreover, causing significant stigma, pain, and suffering to families, this symptom was often erroneously attributed to distant parenting (Bettelheim, 1967). During this time, Leo Kanner, an American psychiatrist, sought to distinguish autism as its own disorder, characterized by a unique set of behaviors, independent of childhood Schizophrenia. Kanner’s 1943 publication, entitled “Autistic disturbances of affective contact,” presented 11 comprehensive case histories of children with characteristics similar to those by which ASD is defined today. Their shared symptoms included social withdrawal, echolalia, the need for sameness/resistance to change, atypical sensory responses, and repetitive behaviors such as spinning and rocking. Kanner rejected the commonly held belief that autism was a product of “cold” child-rearing environments, and instead came to believe that autism was congenital in nature (Baker, 2013; Kanner, 1943). Kanner’s documentation of the common behavioral profiles of this group of patients broadened the definition and understanding of autism as a behavioral disorder.
Interestingly, at the same time that Kanner was completing his work in the United States, Hans Asperger, an Austrian pediatrician, used the term autistic to describe a group of four boys who had traits similar to Kanner’s cohort of patients but who were higher-functioning in terms of cognitive capacities. In his classic “Autistic psychopathology” article published in 1944, Asperger described deficits that were slightly more social in nature in the four boys whom he characterized as “little professors,” a term that was often applied to describe children who met criteria for the later defined Asperger’s Syndrome, which was included in DSM-IV, but is considered part of ASD in DSM-5.
The works of Kanner, Asperger, and Rimland suggested that autism was based in biology and not caused by distant or cold parenting. These early writings laid the groundwork for the emergence of infantile autism as its own disorder in the DSM-III in 1980. Infantile autism in the DSM-III, consisted of the following three major symptom clusters, each of which had to emerge before 30 months of age: lack of responsiveness to others, severe impairments in language development, and “bizarre responses” to aspects of the environment. Additionally, to distinguish infantile autism from childhood Schizophrenia, the authors of the DSM-III included a requirement of an absence of delusions and hallucinations. DSM-III applied a monothetic approach (i.e. an individual had to meet all three diagnostic criteria), and therefore focused on what might now be considered classic autism, as manifested in more severely affected individuals.
The conceptualization of the disorder changed significantly from DSM-III to DSM-III-R (APA, 1987). This version introduced a more developmental emphasis and polythetic criteria (i.e. an individual had to meet a certain minimal number of defining characteristics, but not all symptoms of the diagnostic criteria) in which individuals had to meet only eight of 16 defined criteria. Additionally, the requirement for an age of onset prior to 30 months was removed. The descriptions of the 16 possible symptoms in the DSM-III-R reflected an attempt to enhance diagnostic precision based on the prevailing understandings of the disorder, which were rooted in both the extant research and clinical practice. To meet criteria for the diagnosis, an individual needed to show at least two of five symptoms that reflected evidence of impaired reciprocal social interaction, one of six symptoms that reflected evidence of impaired verbal and nonverbal communication, and one of five symptoms that reflected the presence of restricted and/or repetitive behavior. Further, the authors of the DSM-III-R created an additional category called Pervasive Developmental Disorder – Not Otherwise Specified (PDD-NOS) for children who displayed some of these symptoms but did not meet the full criteria for a diagnosis of autistic disorder. While the given list of symptoms provided a more structured organization of the criteria for the disorder, the addition of PDD-NOS increased the overall flexibility of the application of the diagnosis and increased the number of individuals who met criteria for these disorders (Hansen, Schendel, & Par, 2015).
While DSM-III-R included the addition of PDD-NOS, it was not until the 1990s that Lorna Wing, an English psychiatrist, and Uta Frith, an English psychologist, popularized the term Asperger’s Syndrome. The work of Wing and Frith contributed to another shift in the conceptualization of autism when Asperger’s Syndrome was officially recognized as a distinct subtype of the disorder in the publication of DSM-IV in 1994. The diagnostic criteria for Asperger’s Syndrome were similar to that of autistic disorder, but required typical language development, average cognitive abilities, and average adaptive behavior abilities (other than in social interaction). At this point, clinicians and researchers began to conceptualize autism along a broad continuum or spectrum of functioning levels and abilities (Baker, 2013).
Similar to DSM-III-R, DSM-IV relied on a polythetic approach, such that a diagnosis of autistic disorder required at least six of 12 listed criteria. To receive the diagnosis, an individual was required to evidence at least two of four symptoms of “qualitatively” impaired social interaction, one of four symptoms of “qualitatively” impaired communication, and one of four restricted or repetitive behaviors or interests. Moreover, the age of onset criteria was reinstated: at least one of the behaviors needed to be evident prior to three years of age. The criteria for autistic disorder, PDD-NOS and Asperger’s Syndrome did not change in DSM-IV-TR, published in 2000.
The publication of the DSM-5 (APA, 2013) sparked a great deal of controversy among family members, clinicians, and researchers. It also captured the attention of the general public, as marked changes were made to the criteria and manner in which disorders would be classified. Specifically, multiple disorders are now subsumed within a single autism spectrum disorder classification, a major change from the manner in which disorders were grouped in DSM-IV. In addition, where appropriate, in DSM-5 clinicians are required to provide a qualifier to the ASD diagnosis, which is quantified along a continuum of severity. The qualifier is used to designate the degree of support the individual with ASD requires, ranging from individuals who require minimal support to those who require very substantial support. Additionally, the qualifier helps to describe an individual’s current symptomatology with the recognition that severity may vary by context. The revision committee eliminated the subtypes of Asperger’s Syndrome and PDD-NOS as well as the overarching category of Pervasive Developmental Disorders, replacing these classifications with a single classification termed Autism Spectrum Disorder (Ozonoff, 2012).
This decision created a powerful discourse regarding the loss of an entire group’s identity. For example, Giles (2013) discussed how a culture developed around the diagnosis of Asperger’s Syndrome, and thus meeting criteria for this disorder shaped a “blueprint for social identity” (p. 3). The committee justified their decision of creating a single “autism spectrum disorder” (ASD) diagnosis based on a body of evidence supporting that differentiation of ASD from typical development and other childhood disorders was done reliably and validly, while the distinction between the three subtypes was found to be inconsistent and varied across research sites (Gibbs et al., 2012).
Moreover, in DSM-5 the traditional triad of symptom domains (i.e. social, communication, and atypical/repetitive behaviors) was reduced to a dyad of symptoms by combining social and communication symptoms into a single domain (social communication deficits) to emphasize the social nature of communication symptoms relevant in ASD. In addition, sensory abnormalities were added to the second domain of restricted, repetitive behaviors, interests, or activities (RRBI). Sensory abnormalities were not included in the DSM-IV-TR RRBI criteria. In contrast to the polythetic criteria in the third and fourth editions of the manual, the DSM-5 re-adopted a mixed monothetic and polythetic approach that requires meeting all of the listed social-communicative criteria (i.e., monothetic) that is contrasted with a polythetic approach for RRBI criteria, for which only two of the four defined symptoms must be present to assign a diagnosis. Finally, the specific age of onset was removed so that symptoms of the disorder must be present in infancy or early childhood, recognizing that the full disorder may become apparent in later years as the social demands of interpersonal relations increase.
The development of the new DSM-5 diagnosis of ASD leaves some questions unanswered. Although the majority of individuals who would have met DSM-IV criteria are likely to also meet DSM-5 criteria, there will not be 100 percent concordance. It remains unclear who will gain and who will lose a diagnosis with the revised DSM-5 diagnostic criteria, and what the long-term effects will be on access to services. Revising the organization, criteria, and nomenclature for describing the individuals first identified by Kanner and Asperger as having a unique set of symptoms associated with impairment associated autism is not a new phenomena. The conceptualization of ASD has undergone several shifts over time to accommodate new understandings of the etiology and developmental course of the disorder.
Symptoms
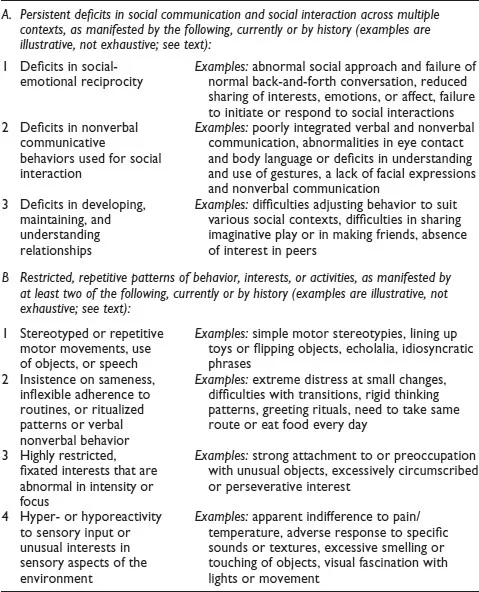
ASD is currently characterized by impairments in an individual’s social communication as well as the presence of RRBIs. Both retrospective and prospective research has informed the current conceptualization of the diagnosis (Ozonoff, 2012). Below, the defining symptoms of ASD, as described in the DSM-5, are explained in detail. The symptoms are divided into two domains: (1) impaired social communication skills (including impaired social-emotional reciprocity, impaired nonverbal communication, and atypical social relationships) and (2) restrictive and repetitive behaviors and interests. See Table 1.1 for DSM-5 descriptions of social communication and social interaction symptoms and restricted, repetitive patterns of behavior, interests, or activities symptoms (APA, 2013).
Table 1.1 Autism Spectrum Disorder DSM-5 Criteria for Social Communication and Restricted and Repetitive Patterns of Behavior, Interests, or Activities
A. Impaired Social Communication Domain
1. Impaired Social-emotional Reciprocity
Starting from a very early age, children with ASD show abnormal social-emotional responses (De Giacomo & Fombonne, 1998; Gillberg et al., 1999; Guinchat et al., 2012; Osterling & Dawson, 1994; Webb & Jones, 2009; Werner, Dawson, Osterling, & Dinno, 2000; Wimpory, Hobson, Williams, & Nash, 2000; Young, Brewer, & Pattison, 2003), including the presence of some or all of the following symptoms: lack of and/or abnormal eye contact or gaze; decreased frequency of looking at others’ faces; lack of interest in playing with other children; preference for playing alone; absence of pointing, giving, and showing objects; and lack of response to social stimuli, such as the child’s own name being called. Such impaired social-emotional responses have been documented as early as within the first six months of life (Maestro et al., 2002). However, prospective studies of high-risk infants (infant-siblings of older children diagnosed with ASD) have revealed that most infants who go on to later receive an ASD diagnosis do not show significant differences in social-emotional responses until the second year of life (Ozonoff et al., 2010). By 12 months of age, some infants later diagnosed ...