
eBook - ePub
Paediatric Obesity
Not only a Weight Concern
Angelo Pietrobelli
This is a test
Buch teilen
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
Paediatric Obesity
Not only a Weight Concern
Angelo Pietrobelli
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
Childhood obesity is increasing, especially in Western Countries. Overweight and obese children are more likely to become obese adolescents and obese adults, with obvious physical and psychosocial consequences, and economic expenditures for Healthcare Systems. Based on the American Academy of Pediatrics (AAP) guidelines, this book provides paediatricians with recommendations and advices for adequate treatment and management of obesity and overweight in young patients. The included BMI-percentile-for-age calculator supplies the right treatment strategy in accordance with AAP guidelines.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Paediatric Obesity als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Paediatric Obesity von Angelo Pietrobelli im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Médecine & Soins infirmiers en pédiatrie. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
Thema
Médecine1 Preface
The rapid rise in obesity prevalence among children is a mirror of the future epidemic of obesity-related medical conditions. Childhood obesity may also be accompanied by health problems that require medical attention at the time of diagnosis. Approximately 60% of overweight youth, including children aged 5 to 10 years, have at least one risk factor for future cardiovascular disease.
As primary health care providers and family pediatricians care for increasing numbers of overweight children, appropriate identification of medical conditions and risks become increasingly important.
The handbook by Pietrobelli, “Pediatric Obesity: not only a weight concern”, provides detailed information for weight management starting from body composition and clinical assessment to comprehensive multidisciplinary treatment. It is fundamental for daily clinical practice to have clear and simple directions for intervention using dietary modification, increased physical activity and behavior therapy. Recent studies indicate that comprehensive interventions that include behavioral therapy along with changes in nutrition and physical activity are the most successful approaches to improving long-term weight control and health status.
Pietrobelli’s timely handbook provides guidance on obesity treatment to practitioners offering a comprehensive approach that is reasonable, feasible, and flexible.
Prof. Steven B. Heymsfield, MD
Executive Director
Pennington Biomedical Research Center
2 Introduction
Obesity is defined by the World Health Organization as “abnormal or excessive fat accumulation that may impair health” [1]. In children and adolescents, obesity represents not only a risk for the well-being of those that are affected, but also a serious health risk. In fact, for the first time in the history of the United States—the country most affected by this real epidemic—children’s life expectancy could be inferior to that of their parents.
Despite the overwhelming evidence of the risks involved, the increase of mean weight is still rising in all Western countries, especially in urban areas. In the United States, the number of overweight adults exceeds that of persons with normal weights, and the levels of obese or overweight people in some European countries are also high.
As shown in Figure 1, Italy has a very troublesome situation with 24% of their children considered obese or overweight. In Denmark, where the situation is not so dramatic, the amount of male adolescents with obesity increased seven times in the final 14 years of the last century.
Causes for the increase of obesity and overweight in the whole population, and particularly in children, which has increased unrestrainedly since the Seventies, can be traced primarily to two factors: diet and physical activity. On the one hand, the great diffusion of technology caused a decrease in physical activity; on the other hand, dietetic habits also changed greatly because of the marketing strategies of alimentary products (e.g., the introduction of snack distributors in the schools, the increase of portion sizes, an increase in the number of fast foods restaurants, and so on).
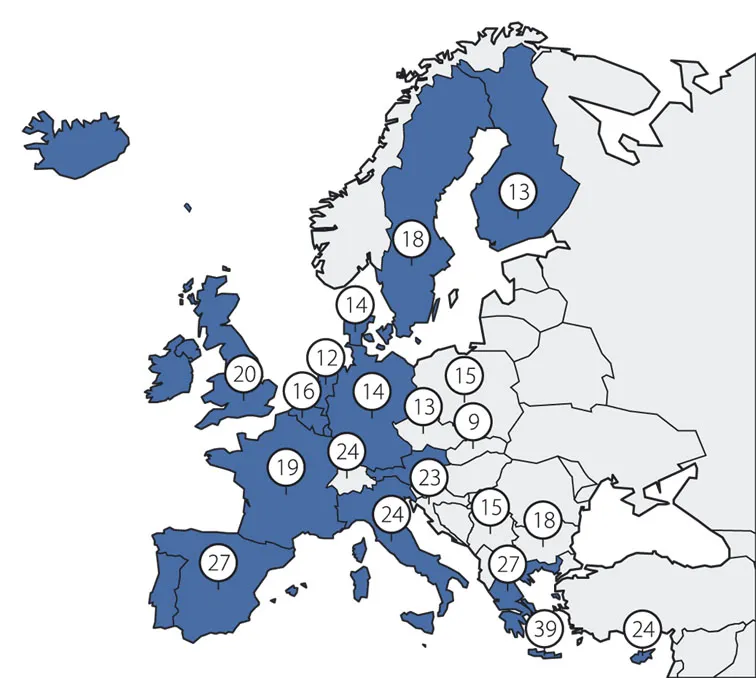
Figure 1. Obesity and overweight prevalence (%) of children in Europe.
At present, it has been calculated that there are 4 million obese children and 16 million overweight children in Italy, with prevalence ranging higher from northern down to southern Italy (Figure 2). The peak of overweight children and adolescents has been registered in the Campania Region, with a prevalence equal to 36%. An obese child has a high probability of becoming an obese adolescent and therefore an obese adult. This fact implies very important health consequences, both from a physical and psycho-social point of view. Cardiovascular risk factors that are already observed in an overweight child tend to persist in adulthood. An overweight adult has an increased risk of insulin resistance, hypertension, hypertriglyceridemia, dyslipidemia, cardiovascular diseases, noninsulin-dependent diabetes, cholecystitis, respiratory difficulties, and even some kinds of tumours [2]. It is therefore easy to understand that the burden of healthcare costs related to obesity is very high, both in terms of resources and logistics.
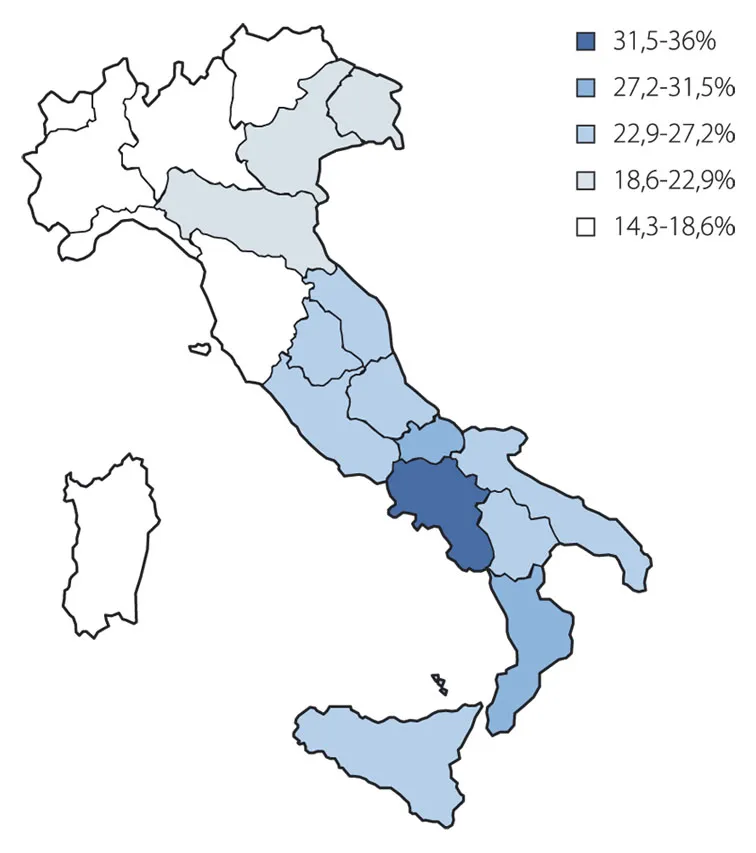
Figure 2. The prevalence of overweight in Italy.
Every year in Italy, obesity-related diseases cost the National Health System 22.8 billion euros, 64% of which is dedicated only to hospital recoveries [3].
With the aim of stemming this epidemic, national and international guidelines have been developed. Among the international guidelines, we can cite the ones of the American Society of Pediatrics, which concern prevention and treatment [4,5]. In Italy, a national Consensus on obesity in children was developed by a joint board composed of members of the Italian Society of Pediatrics (Società Italiana di Pediatria), the Italian Society of Endocrinology and Paediatric Diabetology (Società Italiana di Endocrinologia e Diabetologia Pediatrica), the Italian Society of Paediatric Nutrition (Società Italiana di Nutrizione Pediatrica), the Italian Society of Medicine of Adolescence (Società Italiana di Medicina dell’Adolescenza), and the Italian Society of Preventive and Social Medicine (Società Italiana di Medicina Preventiva e Sociale) [6]. These recommendations represent a major point of reference for the prevention and the management of the disease.
3 The visit
As a general rule, a visit to paediatrics requires additional competencies in the areas of communication and counselling. In the treatment of obesity and overweight, it is important that both the child and his parents are equally involved in the consultation, so that the reasons for the measurements that are executed can be clearly illustrated and the need for a child’s weight surveillance can be fully explained to them, for reasons other than merely esthetical consideration. Because of the value of a person’s physical “looks” in our culture, and because of the common belief that overweight is mostly caused by laziness and lack of will, overweight children and their parents could be embarrassed and ashamed during the visit. Therefore, a clinician should practice patience and sensibility. He should convince the child and his parents that obesity is a chronic disease and that therefore it can be cured. The tone should never be accusatory and the doctor should aim for creating an alliance with the family, finding out behaviours that can be improved, and paying attention to the peculiarities, needs, and difficulties of each single child.
The first step consists of verifying the presence of overweight or obesity; the paediatrician should then evaluate the possible presence of risk factors for obesity, and the existence of comorbidity, always relating the observations to the family context of the child. The frequency of the visits should be decided based on the patient’s characteristics. If there are neither weight abnormalities nor risk factors of comorbidities, doctors should only monitor a child’s weight during routine visits and underline the importance of appropriate eating and exercise behaviour to prevent excess weight.
If an overweight child is noticed, an in-depth examination should be performed, and the subsequent controls should be tighter [5]. Besides the severity of the overweight, the doctor should also schedule the frequency of controls on the basis of the response to treatment, the patient’s age, the presence of risk factors of comorbidities, and motivational factors. In fact, it is important that the physician takes into account the child’s readiness to change as well as that of his parents. During the phase of weight reduction, a consultation should be performed each month (but weekly controls could be necessary in the case of severe obesity or poor compliance to treatment). During the maintenance phase, follow-up visits should be scheduled every six months [5].
3.1 Overweight estimation
The assessment of obesity in the child requires adequate and accurate methods to verify body composition and growth levels. An examination of published articles about obesity in children shows a lack of consensus regarding what is considered “fatness” in the child [7]: despite the trend that has emerged in the last few years, to standardise—as long as possible—methods used to measure overweight, differences in techniques described in clinical trials, to evaluate the amount of fat mass, the presence of overweight and their changes during time, are still present.
Despite the existence of direct methods for measuring body fat—i.e., techniques that allow us to measure the quantity of fat, its distribution, and its composition (computerised tomography, magnetic resonance)—these methods are not used in standard clinical practice because of their excessive costs. The estimate of overweight is therefore usually obtained with indirect methods or anthropometric measurements which, even if not as accurate, are easily applicable and less expensive. They are:
- Body Mass Index (BMI);
- waist circumference and waist/hip circumference ratio; and
- triceps and subscapular thickness.
Currently, BMI percentiles for age as established by the International Obesity Taskforce [8] are also widely used in epidemiological studies. The World Health Organization (WHO) has recently introduced the “Child Growth Standards for children between the ages of 0 and 5 years” [9], and the “WHO Growth References for children between the ages of 5 and 18 years” [10].
Finally, in Italy we usually refer to the growth curves based on height, weight and BMI derived from a study conducted on 70,000 Italian children between the ages of 2 and 20 [11].
Body Mass Index
The Body Mass Index is recognised as a valid measure for the estimation of obesity in a general population.
BMI is defined as the ratio between weight (in kg) and the square of the height (in m2), and is widely used as an index for relatively adiposity. This index, nevertheless, even if widely used for adults, has some limitations in the paediatric population: the interpretation of this datum can, in fact, be difficult in each single child because it can be influenced by age, race and the amount of muscle mass. Using data derived from samples from different countries, Cole and colleagues elaborated on curves used to provide BM...