David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill, David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill
This is a test
This is a test
Buch teilen
534 Seiten
English
ePUB (handyfreundlich)
Über iOS und Android verfügbar
eBook - ePub
Physical Activity and Health
The Evidence Explained
David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill, David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
Physical Activity and Health explains clearly, systematically and in detail the relationship between physical activity, health and disease, and examines the role of exercise in the prevention and management of a wide range of important conditions.
Now in a fully updated and expanded third edition, this is the most complete and engaging textbook on the subject. It offers a balanced examination of the latest evidence linking levels of physical activity with the risk of mortality, cardiovascular diseases, diabetes, obesity, cancer, osteoporosis and dementia. Designed to help the reader evaluate the quality of the evidence, the book includes an invaluable discussion of common study designs and the inherent difficulties of measuring physical activity. It examines the evidence in relation to child and adolescent health, older adults, hazards of exercise, sedentary behaviour, public health policy and, in a new chapter, mental health, and an epilogue considers the emerging evidence regarding the significance of physical activity and COVID-19.
Containing chapter summaries, study tasks, guides to supplementary reading, a glossary of key terms and an abundance of figures and tables, Physical Activity and Health is an essential course text, and important reading for undergraduate, masters and postgraduate research students of sport and exercise science, public health, physical therapy, medicine and nursing.
This third edition is supported by an updated companion website featuring self-test questions, PowerPoint slides, learning activities and website links.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Physical Activity and Health als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Physical Activity and Health von David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill, David J. Stensel, Adrianne E. Hardman, Jason M.R. Gill im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicine & Sports Medicine. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
█Prevalence of physical activity/inactivity worldwide
█Sedentary behaviour
█Therapeutic potential of physical activity
█Costs of physical inactivity
█Definitions of key terms
█Summary
█Study tasks
█Further reading
█References
Early observations
Physical activity and physical fitness have been linked with health and longevity since ancient times. The earliest records of organised exercise used for health promotion are found in China, around 2500 bc. However, it was the Greek physicians of the fifth and early fourth centuries bc who established a tradition of maintaining positive health through ‘regimen’ – the combination of correct eating and exercise. Hippocrates (c. 460–370 bc), often called the Father of Modern Medicine, wrote:
all parts of the body which have a function, if used in moderation and exercised in labours in which each is accustomed, become thereby healthy, well-developed and age more slowly, but if unused and left idle they become liable to disease, defective in growth and age quickly.
Modern-day exercise research began after the Second World War in the context of post-war aspirations to build a better world. Public health was changing to focus on chronic, non-communicable diseases and the modification of individual behaviour. Whilst Doll and Hill worked on the links between smoking and lung cancer, Professor Jeremy Morris and his colleagues set out to test the hypothesis that deaths from coronary heart disease (CHD) were less common among men engaged in physically active work than among those in sedentary jobs. In seminal papers published in 1953, they reported that conductors working on London’s double-decker buses who climbed around 600 stairs per working day experienced less than half the incidence of heart attacks as the sedentary drivers who sat for 90% of their shift (Morris et al. 1953) (Figure 1.1).
Figure 1.1 A London double-decker bus in the 1950s. Jeremy Morris and colleagues compared the incidence of heart attack in sedentary drivers with that in physically active conductors.
Subsequent studies by Morris and others, in particular Morris’s close friend Ralph Paffenbarger in the United States (US), confirmed that the postponement of cardiovascular disease through exercise represents a cause-and-effect relationship. For their contribution, Morris and Paffenbarger were, in 1996, jointly awarded the first International Olympic Medal and Prize for research in exercise sciences.
In the 70 years since Morris’s early papers, research into the influence of physical activity on health has burgeoned. This book is not a comprehensive account of this literature; rather it is an attempt to illustrate its extent, strengths and weaknesses, and to help students understand the process of evaluation of evidence. Our emphasis will be on topics that comprise major public health issues. But first, it is necessary to ‘paint a picture’ of some relevant features of today’s societies.
Modern trends
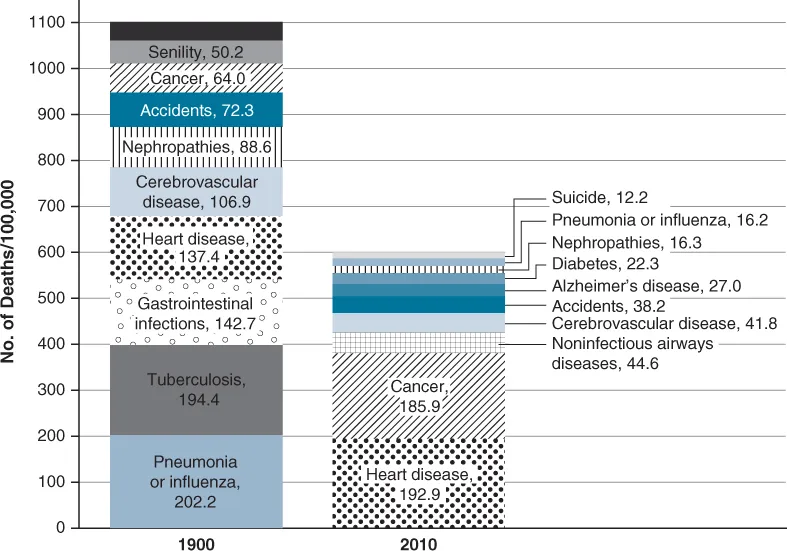
Over the past century or so the predominant diseases afflicting society in most countries have changed from those transmitted through infection (pneumonia, influenza, tuberculosis, diphtheria) to those that are influenced to some extent by lifestyle, e.g. heart disease, cancer, stroke and diabetes (Jones et al. 2012) (Figure 1.2). Of course, there is a genetic element to these diseases (i.e. some people have a greater genetic predisposition to these conditions than others) but three modern trends are exacerbating the prevalence of these lifestyle-related diseases. These are physical inactivity, obesity and the ageing of the population. Before examining physical inactivity, we will briefly survey trends in obesity and ageing.
Figure 1.2 Top ten causes of death in the United States: 1900 versus 2010.
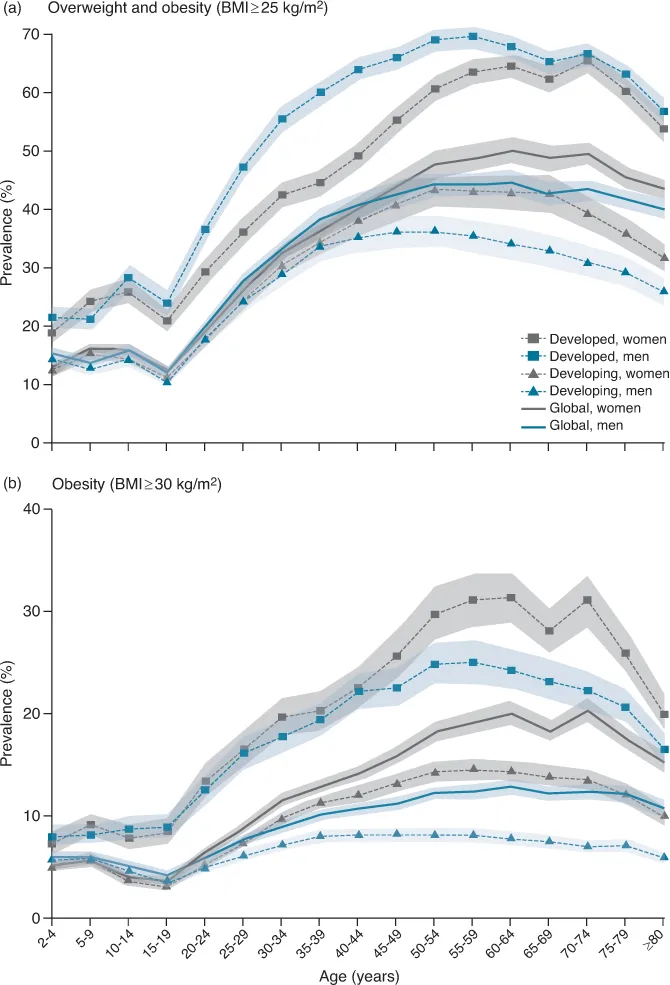
According to research, published in The Lancet in 2014, more than 2.1 billion (approximately 30%) of the world’s population are overweight or obese (Ng et al. 2014) (Figure 1.3). Since 1980 the proportion of adults with a body mass index (BMI) of 25 kg m–2 or greater has increased from 29% to 37% in men and from 30% to 38% in women. In adults, estimated obesity prevalence exceeds 50% in some countries (e.g. more than 50% of men in Tonga and more than 50% of women in Kuwait are estimated to be obese). The prevalence of overweight and obesity has also increased in children and adolescents. In 2013, 24% of boys and 23% of girls in developed countries were either overweight or obese while in developing countries approximately 13% of both boys and girls were overweight or obese. This represents a 47% increase in the worldwide prevalence of overweight and obesity for children since 1980. While there are some signs that the increase in adult obesity prevalence is slowing in developed countries this does not appear to be the case in developing countries. Perhaps more ominous is the observation that there are no national success stories in the struggle to control obesity prevalence over the last three decades (Ng et al. 2014).
Figure 1.3 Prevalence of overweight and obesity and obesity alone, by age and sex, 2013.
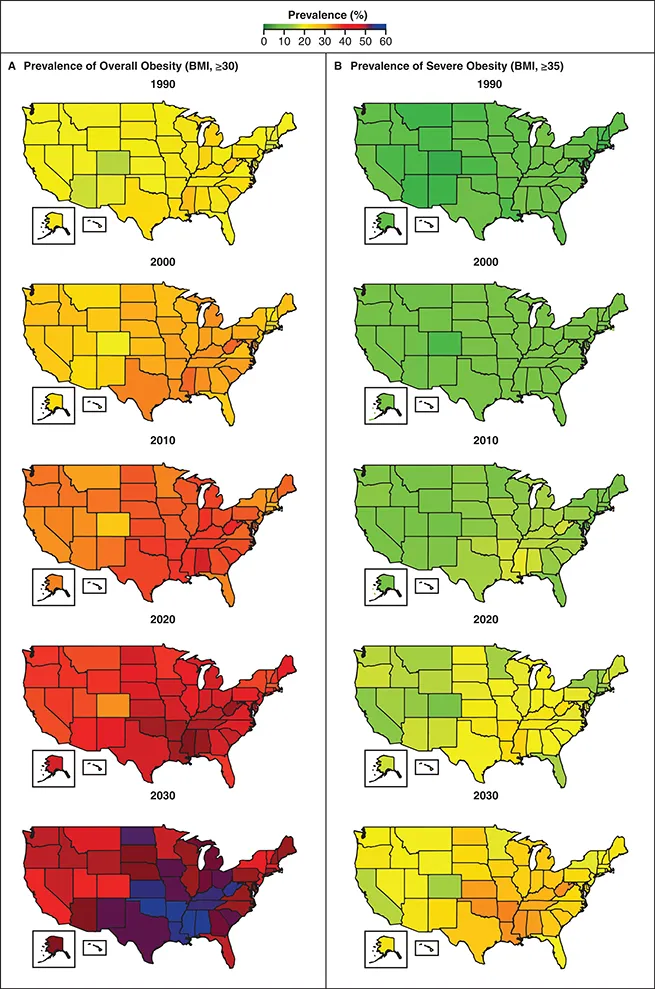
A recent report on adult obesity prevalence in the US (employing data from the Behavioural Risk Factor Surveillance System Survey) estimates that by 2030 nearly one in two American adults will be obese (BMI ≥ 30 kg m–2) and the prevalence of obesity is projected to be higher than 50% in 29 US states. Nearly one in four US adults are predicted to be severely obese (BMI ≥ 35 kg m–2) by 2030 and this is predicted to become the most common BMI category among women (27.6%), non-Hispanic black adults (31.7%) and low-income adults (31.7%) in the US (Ward et al. 2019) (Figure 1.4).
Figure 1.4 Estimated prevalence of overall obesity (Panel A) and severe obesity (Panel B) among adults in each state in the United States, from 1990 through 2030.
Consistent with findings from the US, data from the Health Survey for England suggest that 67% of men and 60% of women in England were overweight or obese in 2018. This includes 26% of men and 29% of women in England who were obese (BMI ≥ 30 kg m–2) and 2% of men and 4% of women who were morbidly obese (BMI ≥ 40 kg m–2). Data from this survey also revealed that 34% of men and 48% of women had a very high waist circumference measurement (>102 cm in men; >88 cm in women), indicating central obesity and placing them at elevated risk of chronic disease (Health Survey for England, 2018 courtesy of the National Centre for Social Research (NatCen) and the Department of Epidemiology and Public Health, University College London, 2019). The Health Survey for England 2018 also reports that 28% of children aged 2 to 15 are overweight or obese, of whom 15% are obese. The National Child Measurement Programme (2019) reports that nearly 10% of children are categorised as obese when starting school, i.e. in reception year (aged 4 to 5 years). As noted by the former chief medical officer for England, Professor Dame Sally Davies, childhood obesity disproportionately affects those living in the most deprived areas and has ‘profound impacts on the health and life chances of children’ (Davies 2019).
The reason there is such concern about obesity is because it is a risk factor for a variety of diseases including cancer, chronic kidney disease, diabetes, hypertension and cardiovascular disease. This will be discussed in greater detail in the coming chapters, but one example here is useful to illustrate the implications of the unrelenting rise in obesity prevalence in recent decades. The disease most closely associated with obesity is type 2 diabetes. In 2008, the global age-standardised adult diabetes prevalence was 9.8% in men and 9.2% in women (up from 8.3% and 7.5% in 1980). Although this includes type 1 diabetes as well as type 2 diabetes, type 2 diabetes accounts for most cases. The estimated number of people with diabetes in 2008 worldwide was 347 million (up from 153 million in 1980). The region with the highest prevalence of diabetes in 2008 was Oceania where 15.5% of men and 15.9% of women had diabetes. Other regions with high diabetes prevalence include South Asia, Latin America and the Caribbean, central Asia, North Africa and the Middle East (Danaei et al. 2011).
Among major developed countries, the US has one of the highest rates of diabetes. Between 1980 and 2010 the number of diagnosed diabetes cases increased from 5.6 million to 20.9 million, representing 2.5% an...