
eBook - ePub
The Art and Science of Facelift Surgery E-Book
Joe Niamtu
This is a test
Buch teilen
- 240 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
eBook - ePub
The Art and Science of Facelift Surgery E-Book
Joe Niamtu
Angaben zum Buch
Buchvorschau
Inhaltsverzeichnis
Quellenangaben
Über dieses Buch
Improved surgical techniques and increasing patient expectations have transformed the field of cosmetic facial surgery, and Art and Science of Facelift Surgery brings you up to speed with today's best and latest procedures. This highly practical resource features a superbly illustrated print reference with step-by-step procedures of each technique. Comprehensive, easy-to-follow instruction from internationally renowned expert Dr. Joe Niamtu helps you achieve optimal outcomes on frequently requested procedures.
- Covers the procedures that today's patients are requesting: male facelift and chin implants, revision facelifts, deep plane facelifts, submandibular gland resection, and many more.
- Includes an abundance of full-color photographs that illustrate surgical steps and before-and-after outcomes, as well as easy-to-follow instruction for each procedure.
- Helps both trainee and practicing aesthetic surgeons attain optimal results and patient satisfaction with every facelift.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist The Art and Science of Facelift Surgery E-Book als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu The Art and Science of Facelift Surgery E-Book von Joe Niamtu im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Médecine & Dermatologie. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
Information
Thema
MédecineThema
DermatologieChapter 1
What is a Facelift? History and Semantics
The word facelift has no standard definition because it means different things to different people including patients and surgeons. One can search the Internet and, just to name a few, find:
- • Full facelift
- • Midfacelift
- • Endoscopic facelift
- • Neck lift
- • Filler facelift
- • Vampire facelift
- • Thread facelift
- • Fast lift
- • Quick lift
- • Lifestyle lift
- • Stem cell facelift
- • Facelift dentures
Unscrupulous marketing and promotion has assigned the word “facelift” to any procedure that may or may not lift the face. If a procedure does lift the face (even several millimeters) should it be called a facelift? More often than not, when anyone names a facelift (after themselves or any person, place, or thing) it reeks of promotion. Very frequently, these “special” facelifts are simply a basic facelift procedure with some spin on part of the procedure. They are usually just rehashed verbiage that surgeons or companies use to gain attention to their specific technique. Also in my experience, these types of surgical facelift attempt to eliminate integral parts of the classic facelift procedure. This may be done because the surgeon does not have the expertise to perform classic facelift (including the Superficial Musculo-Aponeurotic System [SMAS], platysma and SMAS management) or the abbreviated lift may be promoted as “easier”, “medical breakthrough”, “shorter recovery”, “more affordable”, and on and on. Unfortunately, this confuses the public and oftentimes leads to poor choices and disappointment on the part of the surgeon. Please do not misinterpret my intentions in this description, I am not attempting to demean any group, surgeon, or company. My main problem with over-marketed hype is that the patient does not realize the standard. Like anything else in life, if it sounds too good to be true, it probably is. If the word “facelift” was standardized, it would represent the classic cervicofacial rhytidectomy, which is a misnomer in itself. Rhytidectomy means “to excise wrinkles” and that is really not what a facelift does. The word, however, has stood the test of time and usually defines a procedure with incisions in front and behind the ear as well as in the submental region. The classic procedure includes undermining flaps of various lengths in various tissue planes, managing surrounding fat through various procedures, treating the SMAS or deep tissues to provide deep suspension and excising excess skin. In my world (and most of my colleagues') that is what a “facelift” is. If I had to define it further, I would call it an “incisional dissection suspending and excision procedure”. I could call it an IDSEP to be grossly descriptive, but then I would enter the same arena as those promotional re-nomenclature. The incision, dissection, suspension, excision procedure is what I refer to as a “comprehensive facelift”. Bcause the procedure actually affects the neck more than the face, I also refer to the procedure as “face and neck lift”. Otherwise, patients may not realize that a “facelift” also improves the neck. To confuse the issue, some surgeons perform an isolated “neck lift” that only uses posterior auricular incisions. Very few patients are candidates for this truncated procedure and it is uncommon. It is important that patients do not confuse this “necklift” with the actual effects of a conventional, contemporary, comprehensive face and neck lift. In common parlance, a facelift is really a “face and neck lift”.
One of the most confusing names is the “full facelift”. About 60% of my facelift consults lead the patient to ask: “Do you mean I need a full facelift?” I always joke with them and tell them I can do a half facelift instead of a full facelift and they choose which side! I believe the term “full facelift” is a holdover from the days when a coronal browlift accompanied most facelifts. This pretty much gave the patient an incision around the entire face when considering the scalp, preauricular and postauricular and submental incisions. Many patients, especially senior ones, associate a “full facelift” with the past incision fest. Also because many facelifts are performed with other cosmetic procedures such as blepharoplasty, browlift, and facial implants, the definition becomes further vague for the patient.
Besides the negative association of the name, facelift surgery has numerous other negative connotations. Before the days of volume addition in the form of fat, implants, and fillers, many facelifts looked very unnatural. This has to do with several factors. First and foremost was the fact that 40 years ago, most patients waited until they “looked old” to have a lift. Many of these patients had skeletonized faces from senescent volume loss and by pulling the skin tight against a gaunt, skeletal face and adding an often over-corrected coronal browlift, patients often looked very unnatural. Definitely tighter, but not necessarily younger. If there are two historical factors that to this day still stigmatize facelift surgery, they are over correction and the lack of volumization. For some reason, many celebrities (who have access to money, travel, and preferred surgeons) end up with extremely unnatural results that scare off many patients from having surgery.
The natural progression of facelift advancements is also a culprit in the negative connotation of the procedure. Historically, early lifts were performed with small skin excisions only. Later suture suspension was added, but these were still primarily “skin only” lifts. With advancement, the platysma and SMAS were treated which provided more natural and lasting outcomes. Older patients may only be aware of the techniques we now call primitive. Along this historical timeline, there have truly been some trial and error “disasters” that are hard to comprehend now (Fig. 1.1).

Fig. 1.1 I have seen several patients present for consultation with posterior cervical scars from a “facelift” to tighten the face.
In addition, the phrase “there is nothing new under the sun” rings true with facelift surgery. Although many surgeons promote short scar, limited incision facelifts with purse string sutures as new or miraculous, they have, in fact, been around for a century (Fig. 1.2).
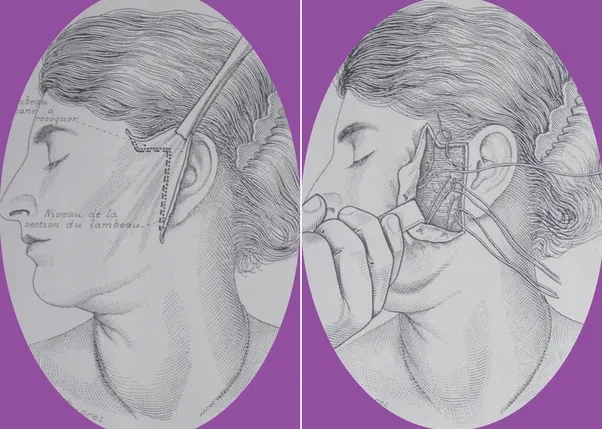
Fig. 1.2 Although limited incision facelifts with purse string sutures are currently promoted by some as “breakthroughs”, they are in fact a centennial procedure. (From Niamtu, J. Cosmetic Facial Surgery, 2nd ed. (2018). Philadelphia, PA: Elsevier. Fig. 3.3. Page 35)
My job is not to attempt to provide the only definition of this procedure and not to condemn those surgeons who perform abbreviated examples of face lifting. On the contrary, many of today's best facelift surgeons started their journey with smaller, simpler procedures and climbed the learning curve. Just as most general surgeons performed an appendectomy before they did a Whipple procedure, cosmetic surgeons walked before they ran. Although I infrequently perform short scar, limited incision facelifts, they do serve a purpose for select patients with minimal aging. In addition to that, these were the first type of facelifts I performed and they served as a great model and practice for progressing into more comprehensive techniques. Small lifts can be a great learning tool.
Small lifts are also an acceptable technique for doctors who may not have extensive surgical training in the head and neck. Some specialties may perform small lifts as the pinnacle of their surgical offering. There is not a problem with this as long as:
- 1. The patient has minimal aging commensurate with a small lift
- 2. The patient understands the limitation of the procedure in anticipated results
- 3. The patient understands the smaller longevity of the procedure
- 4. The patient understands what the small lift “won't do”
If the aforementioned are followed, a small lift on a patient with minor aging may be the perfect fix. If, however, the patient has moderate to advanced aging and they get a small lift, ethical boundaries are breached. I, unfortunately, see many patients who had short scar, (limited incision) procedures without plastysmaplasty who were totally inappropriate candidates (Fig. 1.3). The result and longevity are substandard and they were in no way, shape or form, candidates for an abbreviated lift. They now have to spend the money all over again to have their aging face improved the right way. Again, there is nothing wrong with smaller lifts, as long as the patient has smaller aging. This will be discussed more in the short scar, limited incision chapter in this book.
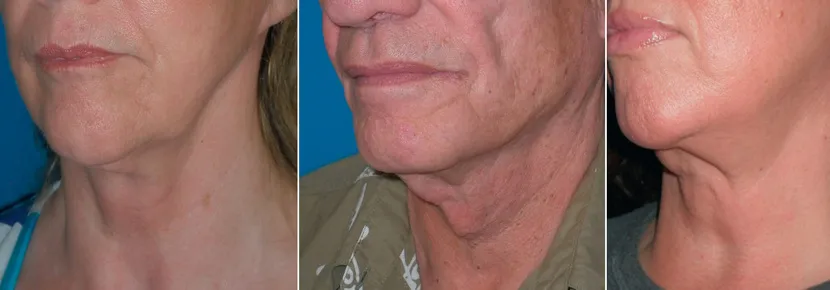
Fig. 1.3 These three patients presented to my office within a year of having a heavily promoted short scar procedure that was touted as a “medical breakthrough”. Unfortunately, these patients were treated with a small lift and need a larger lift, hence the poor postoperative results. (From Niamtu, J. ...