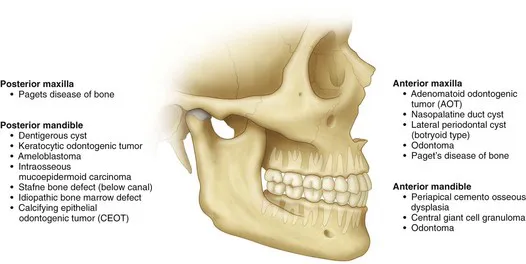
Multilocular Radiolucent Lesion in the Pericoronal Region (Keratocystic Odontogenic Tumor [Odontogenic Keratocyst])
CC
A 20-year-old man is referred for evaluation of a swelling on his right mandible.
Keratocystic Odontogenic Tumor (KCOT)
Keratocystic odontogenic tumors (KCOTs) show a slight predilection for males and are predominantly found in individuals of Northern European descent. The peak incidence is seen between 11 and 40 years of age. Patients with larger lesions may present with pain secondary to infection of the cystic cavity. Smaller lesions are usually asymptomatic and are frequently diagnosed during routine radiographic examination.
The World Health Organization (WHO) has recommended the use of the term keratocystic odontogenic tumor (KCOT), rather than odontogenic keratocyst (OKC), because the former name better reflects the neoplastic behavior of the lesion. Genetically, the lesion shows a repeatable chromosomal abnormality (PTCH gene on chromosome 9q22.3-q31).
HPI
The patient complains of a 2-month history of progressive, nonpainful swelling of his right posterior mandible. (About 65% to 83% of KCOTs occur in the mandible, most often in the posterior body and ramus region. KCOTs account for approximately 3% to 14% of all oral cystic lesions.) The patient denies any history of pain in his right lower jaw, fever, purulence, or trismus. He does not report any neurosensory changes (which are generally not seen with KCOTs).
MHX/PDHX/Medications/Allergies/SH/FH
Noncontributory. There is no family history of similar presentations.
Nevoid basal cell carcinoma syndrome (NBCCS) is an autosomal dominant inherited condition with features that can include multiple basal cell carcinomas of the skin, multiple KCOTs, intracranial calcifications, and rib and vertebral anomalies. Many other anomalies have been reported with this syndrome (Box 1-1). The prevalence of NBCCS is estimated to be 1 in 57,000 to 1 in 164,000 persons.
Box 1-1
Diagnostic Criteria for Nevoid Basal Cell Carcinoma Syndrome
Examination
Maxillofacial. The patient has slight lower right facial swelling isolated to the lateral border of the mandible and not involving the area below the inferior border. The mass is hard, nonfluctuant, and nontender to palpation (large cysts may rupture and leak keratin into the surrounding tissue, provoking an intense inflammatory reaction that causes pain and swelling). There are no facial or trigeminal nerve deficits (paresthesia of the inferior alveolar nerve would be more indicative of a malignant process). The intercanthal distance is 33 mm (normal), and there is no evidence of frontal bossing. His occipitofrontal circumference is normal (an intercanthal distance [the distance between the two medial canthi of the palpebral fissures] of greater than 36 mm is indicative of hypertelorism, and an occipitofrontal circumference greater than 55 cm is indicative of frontal bossing; both can be seen with NBCCS).
Neck. There are no palpable masses and no cervical or submandibular lymphadenopathy. Positive lymph nodes would be indicative of an infectious or a neoplastic process. A careful neck examination is paramount in the evaluation of any head and neck pathology.
Intraoral. Occlusion is stable and reproducible. The right mandibular third molar appears to be distoangularly impacted (KCOTs do not typically alter the occlusion). The interincisal opening is within normal limits. There is buccal expansion of the right mandible, extending from the right mandibular first molar area posteriorly toward the ascending ramus. Resorption of bone may include the cortex at the inferior border of the mandible, but this is observed at a slower rate than in intermedullary bone, which is less dense. For this reason, KCOTs characteristically extend anteroposteriorly than buccolingually. This pattern of expansion into less-dense bone explains why maxillary KCOTs show more buccal than palatal expansion and often expand into the maxillary sinus. There is no palpable thrill or audible bruit, both of which are seen with arteriovenous malformations. The oral mucosa is normal in appearance with no signs of acute inflammatory processes.
Thorax-abdomen-extremity. The patient has no findings suggestive of NBCCS (e.g., pectus excavatum, rib abnormalities, palmar or plantar pitting, and skin lesions; see Box 1-1).
Imaging
A panoramic radiograph is the initial screening examination of choice for patients presenting for evaluation of intraosseous mandibular pathology (10% to 20% of KCOTs are incidental radiographic findings). This provides an excellent overview of the bony architecture of the maxilla, mandible, and associated structures. CT scans can be obtained when large lesions are found. CT scans are valuable in that they provide additional information, such as the proximity of adjacent structures (e.g., the mandibular canal), the integrity of cortical plates, and the presence of perforations into adjacent soft tissues. CT scans provide accurate assessment of the size of the lesion and can demonstrate additional anatomic details (or lesions) that do not appear on panoramic radiographs.
A CBCT scan is appropriate for the evaluation of this lesion. Given its higher resolution, lower radiation dose (approximately 20% of the radiation of a conventional [helical] CT ), and lower cost, a CBCT can replace helical CT for evaluation and follow up of such a lesion. The CBCT scan can also be used to create a stereolithic model of the area of interest.
It has been demonstrated that T2-weighted magnetic resonance imaging (MRI) can detect KCOTs in 85% of new cases with a readily recognizable pattern. However, the use of MRI for management of suspected OKCs is not routine.
In this patient, the panoramic radiograph reveals a large, multilocular radiolucent lesion with possible displacement of the right mandibular third molar (Figure 1-2). T...