Since its recognition as the first specialty of dentistry, the practice of orthodontics has been influenced by the development of new materials, techniques, bracket designs and prescriptions, appliances, and software. However, never before has there been as revolutionary a change as digitization. Digitization and automation are transforming the entire landscape of how orthodontics is practiced, and the consequence is the "do it yourself" concept. With the technology available today with intraoral scanning, CBCT imaging, and CAD software, we can create the virtual patient and manipulate dental models virtually. Not only does this enable better and more precise treatment planning, but it also facilitates better communication with the patient. Perhaps most exciting is that it permits in-house designing and printing of the majority of orthodontic appliances. This book describes the current digital technology that is used in orthodontics, including volume and surface scanning, 3D printing, CAD software, and artificial intelligence, before delving into a "design it yourself" guide presenting the application of this technology in all aspects of orthodontic treatment. It describes all the necessary technologic ingredients to be used in a self-sufficient digital orthodontic clinic, and it focuses on the in-house design and production of tailor-made appliances by digitally diagnosing and evaluating the virtual patient and then creating an individualized treatment plan. Now you can design your own expanders, retainers, clear aligners, brackets, indirect bonding trays, and even wires with a wire-bending robot. It is incredible what technology has to offer; we just have to have the courage to learn and experiment with it. For the benefit of our patients, the challenge is laid.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist DIY Orthodontics als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu DIY Orthodontics von Nearchos Panayi im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medizin & Kieferorthopädie. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
“Do it yourself” (DIY) orthodontics is becoming requisite in modern orthodontic practice. Nevertheless, this book is titled Design It Yourself Orthodontics in order to differentiate it from the “doctorless” direct-to-patient appliances offered online or at shopping mall kiosks.
Technology and 3D software have irrevocably changed the way modern orthodontics is managed and administered. Printed models are eliminating poured plaster casts, appliances can be designed and printed with computer-assisted hardware and software, and tooth movements can be simulated and staged digitally to increase their accuracy and predictability.
Digitization converts real-world information into digital data that can be presented on a computer screen. Volume scanning and surface scanning of the dental arches and the face are transferred to dedicated orthodontic software to build the “virtual patient” for orthodontic diagnosis, tooth movement simulations, and treatment planning.
Artificial intelligence (AI), currently in its initial stages, holds promise in becoming a tool for orthodontic diagnosis and treatment outcome predictions. It also has the potential to assist in defining appropriate treatment options for a specific patient, as well as predicting tendencies of relapse. Furthermore, AI can be a valuable research tool. Blockchain assemblies are described herein that could be a digital tool to connect an infinite number of orthodontic clinicians without a centralized server as a network. This could become a window for participants to view treatment examples, digital appliances, radiographs, etc, without violating patient or doctor privacy.
Dentists and orthodontists can at times be intimidated by mathematics, physics, and technology, which are related to forces and appliance design. Technologic understanding is a time-consuming process with a learning curve that can deter the orthodontist from getting involved. A familiar work pattern and acceptance of a particular appliance serve to create a comfort zone for every clinician. The introduction of a disruptive technology may upset this pattern and disturb the established workflow. Nevertheless, avoidance of these technologies will be to the disadvantage of the practitioner. The longer the delay in integrating these technologies, the greater the learning curve in implementing them. As Darwin stated, it is not the strongest of the species that survives nor the most intelligent—it is the one that is most adaptable to change.
The versatility of digital applications has enabled increased control and greater independence within our clinical settings. This trend has justified the inception of many companies that recognize the need for tools to design and plan individualized appliances according to each clinician’s vision for each case, and to enable modifications as needed during the treatment. These tools include multifunctional orthodontic software for virtual patient analysis, treatment simulation, patient education, treatment planning, and smile design. Other software offers the ability to design and create in-house orthodontic aligners, indirect bonding (IDB) trays, customized bands, appliances, and orthognathic surgical splints, etc. 3D printer companies have recognized the application of their technology in dentistry and orthodontics, and new biocompatible printing resins are continuously under development and being introduced in the market for use.
The younger generations of orthodontists and dentists, while certainly less clinically experienced, are naturally better informed as to these technologies because their emergence into the field parallel one another. Older, more experienced clinicians generally are slow to adopt new technologies due to the apprehension created by the disturbance in established principles and the apparent complexity new technology introduces. Young or old, inexperienced or experienced, all clinicians need sources that enable them to accept new technologies and overcome barriers so they can realize their own innovation.
It needs to be understood that technology is not a replacement for the process of coalescing the appropriate diagnostic information into a patient-specific treatment plan. Digital technology can only serve as an assistant, not the master in orthodontic treatments. Ironically, it is the more clinically experienced category of clinicians that can maximize the potential of these tools; however, their aversion to the changes brought by technology has left this potential unrealized. Also, knowledge of new technology should not give the impression in young dentists and orthodontists that it is sufficient for a satisfactory orthodontic treatment result.
This book, as stated in its title, covers the topic of DIY orthodontics from the simple design of expansion and cast/printed appliances using dedicated computer-aided design (CAD) orthodontic software to unique printed appliances designed by general CAD engineering software. As the reader will notice, such tools enable the orthodontist to directly design appliances that cannot be created with any other software. Indirect bonding with digital preparation is thoroughly described with the add-on of a special IDB process that is undertaken upon digital setup. In-house design of customized lingual braces is presented together with an in-house wire-bending robot, for both lingual and labial archwires.
In-house aligner design is presented using uncomplicated software, an aspiration that is currently central in orthodontics. Furthermore, industry efforts to produce a biocompatible material and technique to directly print clear aligners are discussed in these pages and, together with the applications for AI, are the frontiers in the integration of technology into clinical orthodontics.
One of the most revolutionary chapters of this book describes in-house custom bracket design and printing using a new software called UBrackets. This enables the operator-driven design and building of customized orthodontic bracket bases using composite resin on orthodontic brackets. In addition, as a second software option, the orthodontist can use the software’s bracket library to print fully customized brackets. Volume scanning, surface scanning, 3D printing, and AI are covered in separate chapters. A full overview of the digital office workflow is also covered in detail.
To my knowledge, there is currently no similar compilation of these undeniably important aspects of the modern practice of orthodontics. This does not surprise me because the majority of what is described in this book was not in existence even 5 years ago. The importance of a book such as this is highlighted by the frequency at which new companies and products are popping up on the market, offering new ideas and tools to enable simplification of clinical tasks and broaden our professional lives with new and exciting opportunities.
The authors contained in this book are recognized clinicians and researchers whose reputations and contributions are highly regarded. Each presents their respective topic in a well-written, comprehensive, but very readable manner. All the material appearing in this book is not only topical but also extremely up to date with several items receiving initial exposure in these pages. The text and visual presentations complement each other and engender a flowing and enjoyable reading experience of a cutting-edge group of topics.
The biology of tooth movement and the biomechanics applied to do so are constants within orthodontics. Yet with simple DIY tools, the modern clinician can visualize and simulate treatment, and, most importantly, sustain maximum control of the progress of any given treatment. Furthermore, DIY tools facilitate the ability to modify treatment as and when needed without being limited or dependent on outsourced laboratories and/or commercial companies.
The highly innovative nature of this book is sure to make it standard for every orthodontic office. It will go a long way in helping today’s clinicians immerse themselves in this fascinating era, which will certainly become the “new normal” in every clinic.
2
CBCT in Orthodontics
Apostolos I. Tsolakis Christos Angelopoulos Nearchos C. Panayi Kostas Tsiklakis
CT and CBCT Historical Perspective
Cone beam computed tomography (CBCT) is undoubtedly the most significant diagnostic imaging advancement in maxillofacial imaging in the last 25 years.1,2 Sir Godfrey N. Hounsfield invented computed tomography (CT) in 1972, for which he received the Nobel Prize in Medicine in 1979; however, the principles of tomosynthesis were described in 1934 and provided the theoretical basis of the integration of multiple planar images.3–6
The first patent application for a maxillofacial CBCT was submitted in Italy in 1995 by Attilio Tacconi and Piero Mozzo. This led to the commercial development of the first available CBCT—NewTom DVT 9000. Presently, more than 60 CBCT brands are available, the majority of which offer multiple options to the practitioner, including hybrid panoramic units to a full maxillofacial unit with or without a cephalometric unit.
Basics of CBCT
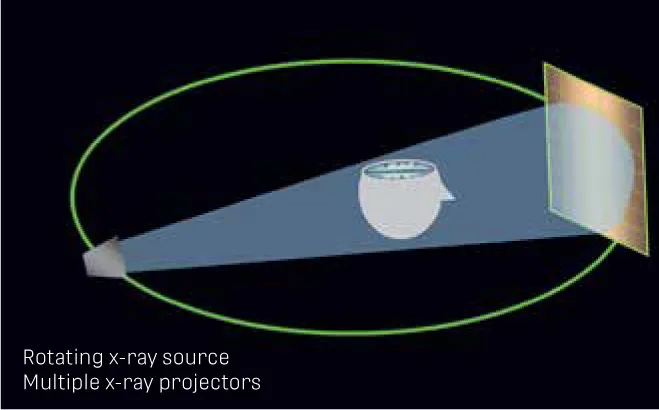
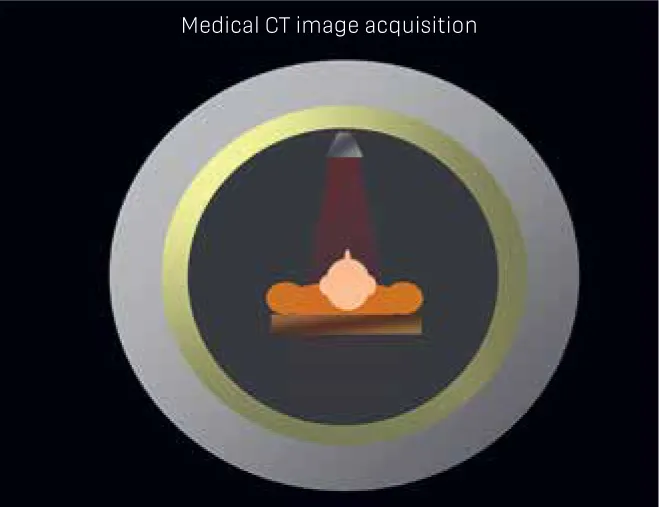
CBCT imaging is accomplished by rotating an x-ray source and a detector around the region of interest (ie, the patient; Fig 2-1). Radiation is emitted by the x-ray source passing through the patient in a cone-shaped beam to the x-ray detector on the opposite side, with the range of the arc employed being 180 to 360 degrees. During the exposure, hundreds of sequential planar projection images are acquired. In contrast, the CT machine consists of a fan-shaped x-ray beam with a simultaneous translation of the patient table and rotation of the x-ray source and detector, resulting in a helical trajectory (Fig 2-2).
Fig 2-1 A rotating x-ray source, a flat panel detector, and a conical beam are the key components of the CBCT image acquisition process. The x-ray tube completes a full rotation around the patient’s head, producing multiple exposures.
Fig 2-2 Medical CT image acquisition involves a thin fan-shaped rotating beam, a ringlike array of detectors (yellow ring), and a supine patient. The x-ray source scans the area of interest with multiple rotations, collecting x-ray attenuation data.
The basic parts of a CBCT are the following7,8:
• An x-ray generator
• An x-ray detector that must be able to capture multiple basic images
• A powerful computer and software able to process all the acquired image data
• Appropriate image acquisition and integration algorithms
In order to transform a series of 2D multiple planar images (which are captured by the 2D x-ray area detector) to a 3D volume image, a cone beam reconstruction image procedure must be performed. In other words, 3D volume reconstruction software turns a series of 2D acquired images into a 3D volume image. The most popular reconstruction scheme for cone beam projections is the FDK (Feldkamp-Davis-Kress). CBCT provides an alternate method of volume scanning, allowing a fast acquisition of data in an in-office mode. CBCT units use an image intensifier or a flat panel detector as the image detector. The larger the detector, the bigger the field of view (FOV), and as a result the better the imaging; however, this increases the cost of the CBCT unit.
An important factor in the quality of the x-ray detector is the pixel size it detects, because this determines radiographic resolution and subsequently the CBCT image quality. A detector with a small pixel size increases the resolution of the acquired imag...