
Abdominal-Pelvic Imaging
200 Cases (Common Diseases): US, CT and MRI
Ammar Haouimi
- 218 Seiten
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
Abdominal-Pelvic Imaging
200 Cases (Common Diseases): US, CT and MRI
Ammar Haouimi
Über dieses Buch
Maybe we have an obsession for cases, but when we were resident in radiology, we loved to learn especially from cases not only because they are short, exciting and fun, similar to a detective story in which the aim is to get to 'the bottom' of the case, but also because, in the end, that's what radiologists are faced with during their daily work.
The topics covered in the book represent the common and important diseases encountered in abdominal and pelvic imaging. The material presented for each case provides a thorough and comprehensive description of the disease entity, enabling the radiologist or the clinician to develop a clear concept of the entity through the different imaging modalities that are present. What is interesting in this book is one case per page. The book can be used as a means of rapid revision of a large number of cases in a short time or as test of knowledge by masking the radiological description and diagnosis and trying by using the clinical data and radiological images to describe first the pathology then propose a diagnosis.
Häufig gestellte Fragen
Information
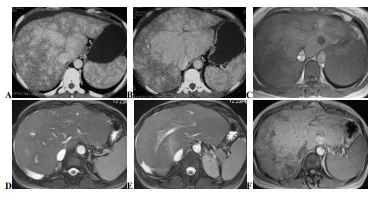
Case 1
-
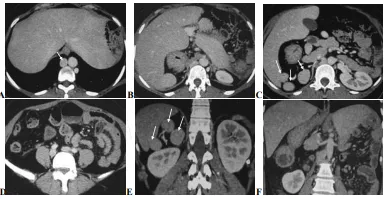
Enhanced CT scan, axial (A, B) and MR scan, axial T1 (C), axial T2 fat saturation (D, E) and post-contrast axial T1 (F) images. On CT images, the liver is enlarged with hypertrophied caudate lobe: mottled enhancement with prominent enhancement of the central liver and decreased enhancement of the liver periphery (nutmeg liver). The areas of decreased enhancement are due to decreased portal flow, hepatic congestion and ischemia. Non-visualisation of the hepatic veins. The MR sequences show the same appearances with homogeneous liver on T2 and enhancement of the central liver (the caudate lobe enhances normally as it has a separate draining vein directly into the inferior vena cava) with decreased signal intensity of the atrophied liver periphery. The IVC is patent. Note mild ascites.
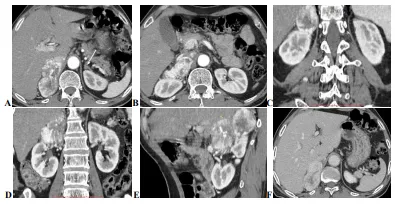
Case 2
-
Enhanced abdominal CT scan, post-contrast arterial phase axial (A, B) / coronal and sagittal reconstruction (C, D, E) and post-contrast portal phase axial (F) images reveal a well-defined lobulated right suprarenal mass with intense and heterogeneous enhancement and prominent surrounding vessels on arterial phase and rapid washout on portal phase. Note the IVC is displaced anteriorly and the upper pole of the kidney posteriorly. The left adrenal gland appears normal in size and shape (arrow image A).
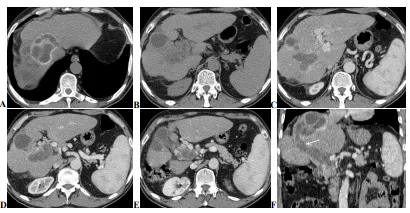
Case 3
-
Pre-(A, B) and post-contrast (C, D, E) abdominal CT scan with coronal reconstruction (F) images showing a dysmorphic liver (past history of surgery for hydatid cysts) with hydatid cysts located in the segments, VIII/VII (CE4 and CE3A, WHO classification) and V (CE3 A, WHO classification). The portal vein and its right branch are dilated, containing germinative membranes and other cyst contents with evidence of fistulous tract between the hydatid cyst located in the segment VIII and dilated right branch of portal vein (arrow in F). Note the presence of tortuous venous structures around the thrombosed portal vein indicating portal cavernoma. The spleen was moderately enlarged with dilated splenic vein (extra-hepatic portal hypertension).
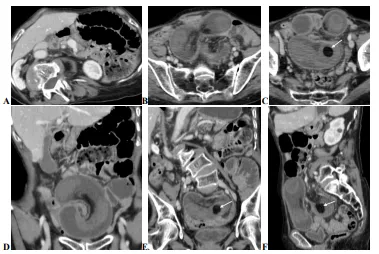
Case 4
-
Enhanced Abdominal CT scan, axial (A, B, C) with coronal / sagittal reconstruction (D, E, F) images showing a sausage-shaped mid-pelvic mass with central area containing mesenteric fat and vessels indicating intussusception. Distal within this mass there is a well-defined fatty-density lesion (arrow images, C, E and F) representing a lipoma. Note proximal small bowel dilatation.
Case 5
-
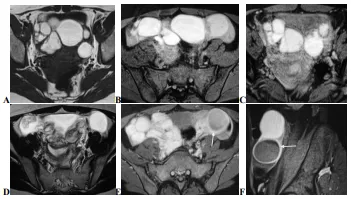
MR scan, axial T1 (A), T1 fat saturation (B, C), axial T2 (D) and post-contrast axial / sagittal T1 fat saturation (E, F) images showing multiple and bilateral well-circumscribed contiguous ovarian cystic lesions of high signal intensity on T1 and T1 fat saturation, low signal intensity on T2 with no peripheral enhancement after gadolinium administration (endometriomas). Both ovaries are closed up due to interovarian adhesions (Kissing ovaries). Note that the left ovary shows also another cystic lesion of high signal intensity on T1 and T2 with peripheral regular enhancement after gadolinium administration (haemorrhagic cyst, arrow in E and F). The uterus was normal.
Case 6
-
Enhanced abdominal CT scan, axial (A, B, C, D) with coronal reformatted (E, F) images. The liver is in midline (or bridging liver) with stomach on the right side. Three splenules are seen on the right below the liver (arrows in C and E) with no splenic structure seen in the left hypochondrium. Note an interruption of the inferior vena cava with azygous continuation of the IVC (arrow in A). The head and the corporeo-caudal region of the pancreas are on the right, giving the appearance of a lying V (image C) with Preduodenal position of the portal vein. The duodenojejunal junction does not cross the midline; it should be located on the same side of the body as the stomach and approximately at the level of the duodenal bulb, indicating associated intestinal malrotation.