With each passing decade, more research is done on GBR, and more surgeons begin adopting this practice with incredible results. Prof Daniel Buser has assembled a team of the top names in implant surgery to put together a comprehensive guide on the materials, indications, techniques, timing, and results of GBR. The book begins with the science of bone regeneration, describing how bone and soft tissue will react and behave under different circumstances, before delving into the different methods and uses of GBR based on the presenting scenario. How to properly time and stage grafting, implant, and prosthetic therapy is a major focus. Case examples are presented documenting each patient's bone regeneration from start to finish, frequently with long-term follow-ups of 10 years or more. Emphasis is given to incision technique and flap design; the selection, handling, and placement of barrier membranes; the combination of membranes with autogenous bone grafts and low-substitution bone fillers; and aspects of wound closure. This book offers solutions for those who want to begin providing implants to a wider range of patients, for GBR veterans who want to refine their skills and practice more advanced techniques, and for implant surgeons who want to keep up to date with the most current research and technology in GBR.
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist 30 Years of Guided Bone Regeneration als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu 30 Years of Guided Bone Regeneration von Daniel Buser im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medicine & Dentistry. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
The Development of Guided Bone Regeneration Over the Past 30 Years
Daniel Buser, DDS, Dr med dent
Modern implant dentistry based on the concept of osseointegration recently celebrated its 50th birthday.1 The tremendous progress made in the rehabilitation of fully and partially edentulous patients is based on fundamental experimental studies performed by two research teams. One team was located in Sweden and headed by Prof P-I Brånemark from the University of Gothenburg; the other was located in Switzerland and headed by Prof André Schroeder from the University of Bern. In the late 1960s and 1970s, the two research groups independently published landmark papers describing the phenomenon of osseointegrated titanium implants.2–4 An osseointegrated implant was characterized by direct apposition of living bone to the implant surface.5–7
In the early phase of this development, several prerequisites were identified for osseointegration to be achieved.2,3 Some of these have been revised over the past 50 years; others are still considered important. In order to achieve osseointegration, the implant must be placed using a low-trauma surgical technique to avoid overheating the bone during preparation of a precise implant bed, and the implant must be inserted with sufficient primary stability.5,8 When these clinical guidelines are followed, successful osseointegration will predictably occur for nonsubmerged titanium implants (single-stage procedure) as well as for submerged titanium implants (two-stage procedure), as demonstrated in comparative experimental studies.9,10
When clinical testing of osseointegrated implants first began, the majority of treated patients were fully edentulous. Promising results were reported in retrospective studies.11–13 Encouraged, clinicians increasingly began using osseointegrated implants in partially edentulous patients, and the first reports on this utilization were published in the late 1980s and early 1990s with promising short-term results by various groups.14–18 As a consequence, single-tooth gaps and distal extension situations have become more and more common indications for implant therapy in daily practice. Today, these practices dominate in many clinical centers.19–21
One of the most important prerequisites for achieving and maintaining successful osseointegration is the presence of a sufficient volume of healthy bone at the recipient site. This includes not only sufficient bone height to allow the placement of an implant of adequate length, but also a ridge with sufficient crest width. Clinical studies in the 1980s and 1990s showed that osseointegrated implants lacking a buccal bone wall at the time of implant placement had an increased rate of soft tissue complications and/or a compromised long-term prognosis.22,23 To avoid increased rates of implant complications and failures, these studies suggested that potential implant recipient sites with insufficient bone volume should either be considered local contraindications for implant placement or should be locally augmented with an appropriate surgical procedure to regenerate the local bone deficiency.
During these early decades, several attempts were made to develop new surgical techniques to augment local bone deficiencies in the alveolar ridge in order to overcome these local contraindications for implant therapy. The proposed techniques included vertical ridge augmentation using autogenous block grafts from the iliac crest in extremely atrophic arches,24,25 sinus floor elevation procedures in the maxilla,26–28 the application of autogenous onlay grafts for lateral ridge augmentation,29–31 or split-crest techniques such as alveolar extension plasty.32–34
During the same period, in addition to these new surgical techniques, the concept of guided bone regeneration (GBR) with barrier membranes was introduced. Based on case reports and short-term clinical studies, various authors reported first results with this membrane technique for the regeneration of localized bone defects in implant patients.35–40
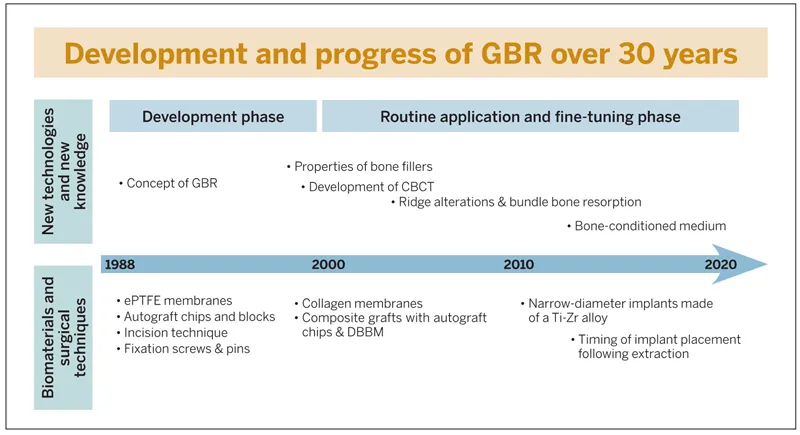
This textbook will provide an update on the biologic basis of the GBR technique and its various clinical applications for implant patients. Clinical experience with GBR in daily practice now spans 30 years. These 30 years can be divided into a development phase and a phase of routine application with extensive efforts to fine-tune the surgical procedure (Fig 1-1). The focus was on improving the surgical technique, expanding the range of applications, improving the predictability for successful outcomes, and reducing morbidity and pain for the patients.
Fig 1-1 Development of GBR over 30 years since the late 1980s. ePTFE, expanded polytetrafluoroethylene; DBBM, deproteinized bovine bone mineral; Ti-Zr, titanium-zirconia
Development Phase of GBR
The use of barrier membranes for implant patients was certainly triggered by the clinical application of barrier membranes for periodontal regeneration, called guided tissue regeneration (GTR). GTR was first developed in the early 1980s by the group led by Nyman et al.41,42 The initial studies were performed with Millipore filters, which had already been used in experimental studies in the late 1950s and 1960s for the regeneration of bone defects.43–45 However, these studies had no impact on the development of new surgical techniques to regenerate localized defects in the jaws, since the potential of this membrane application was probably not recognized at that time.
The two papers by Nyman et al41,42 in the field of GTR, both of which demonstrated successful treatment outcomes of GTR procedures, were received with great interest and led to increased research activities in the mid to late 1980s.46–49 These studies were already being performed with expanded polytetrafluoroethylene (ePTFE), which is a bioinert membrane and became the standard membrane for GTR and GBR procedures during the development phase of both techniques. The use of ePTFE membranes for bone regeneration was initiated in the mid 1980s by the group of Dahlin et al, who performed a series of preclinical studies.50–52 These studies confirmed the concept that the application of an ePTFE membrane established a physical barrier that separated the tissues and cells that could potentially participate in the wound healing events inside the secluded space. The barrier membrane promoted the proliferation of angiogenic and osteogenic cells from the marrow space into the bone defect without interference by fibroblasts. These events were nicely demonstrated by Schenk et al53 in a landmark experimental study in foxhounds. The current biologic understanding of wound healing events in membrane-protected bone defects is presented in detail in chapter 2 of this textbook.
The use of ePTFE membranes for GBR procedures started in the late 1980s. The main objective was to achieve regeneration in peri-implan...