This practical handbook provides detailed guidelines on prescribing drugs in all classes and for a wide variety of diseases and disorders during pregnancy, with numerous boxes and tables to assist understanding.
CONTENTS: Introduction to Drugs in Pregnancy * Antimicrobials during Pregnancy: Bacterial, Viral, Fungal, and Parasitic Indications * Cardiovascular Drugs during Pregnancy * Endocrine Disorders, Contraception, and Hormone Therapy during Pregnancy: Embryotoxic versus Fetal Effects * Antiasthma Agents during Pregnancy * Anesthetic Agents and Surgery during Pregnancy * Antineoplastic Drugs during Pregnancy * Analgesics during Pregnancy * Anticonvulsant Drugs during Pregnancy * Psychotropic Use during Pregnancy * Antihistamines, Decongestants, and Expectorants during Pregnancy * Nutritional and Dietary Supplementation during Pregnancy * Use of Dermatologics during Pregnancy * Drug Overdoses during Pregnancy * Miscellaneous Drugs during Pregnancy: Tocolytics, Immunosuppressants, and Biologic Therapeutics * Substance Abuse during Pregnancy * Online Support Material
Häufig gestellte Fragen
Wie kann ich mein Abo kündigen?
Gehe einfach zum Kontobereich in den Einstellungen und klicke auf „Abo kündigen“ – ganz einfach. Nachdem du gekündigt hast, bleibt deine Mitgliedschaft für den verbleibenden Abozeitraum, den du bereits bezahlt hast, aktiv. Mehr Informationen hier.
(Wie) Kann ich Bücher herunterladen?
Derzeit stehen all unsere auf Mobilgeräte reagierenden ePub-Bücher zum Download über die App zur Verfügung. Die meisten unserer PDFs stehen ebenfalls zum Download bereit; wir arbeiten daran, auch die übrigen PDFs zum Download anzubieten, bei denen dies aktuell noch nicht möglich ist. Weitere Informationen hier.
Welcher Unterschied besteht bei den Preisen zwischen den Aboplänen?
Mit beiden Aboplänen erhältst du vollen Zugang zur Bibliothek und allen Funktionen von Perlego. Die einzigen Unterschiede bestehen im Preis und dem Abozeitraum: Mit dem Jahresabo sparst du auf 12 Monate gerechnet im Vergleich zum Monatsabo rund 30 %.
Was ist Perlego?
Wir sind ein Online-Abodienst für Lehrbücher, bei dem du für weniger als den Preis eines einzelnen Buches pro Monat Zugang zu einer ganzen Online-Bibliothek erhältst. Mit über 1 Million Büchern zu über 1.000 verschiedenen Themen haben wir bestimmt alles, was du brauchst! Weitere Informationen hier.
Unterstützt Perlego Text-zu-Sprache?
Achte auf das Symbol zum Vorlesen in deinem nächsten Buch, um zu sehen, ob du es dir auch anhören kannst. Bei diesem Tool wird dir Text laut vorgelesen, wobei der Text beim Vorlesen auch grafisch hervorgehoben wird. Du kannst das Vorlesen jederzeit anhalten, beschleunigen und verlangsamen. Weitere Informationen hier.
Ist Drugs and Pregnancy als Online-PDF/ePub verfügbar?
Ja, du hast Zugang zu Drugs and Pregnancy von Bertis B. Little im PDF- und/oder ePub-Format sowie zu anderen beliebten Büchern aus Medizin & Medizinische Theorie, Praxis & Referenz. Aus unserem Katalog stehen dir über 1 Million Bücher zur Verfügung.
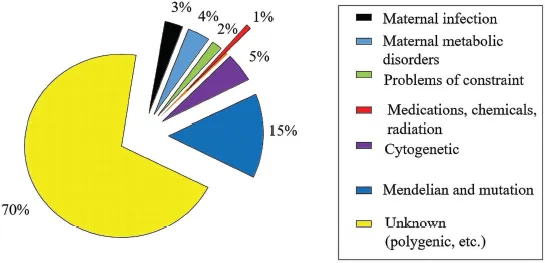
Approximately 3.5–5 percent of live-born infants have a birth defect when examined at birth or neonatally (Polifka and Friedman, 2002), and this is termed the background population risk for congenital anomalies. The prevalence of birth defects may normally be 8 percent, according to a British Columbia universal disease registry (Baird et al., 1989). Estimated teratogenic causes of birth defects (Figure 1.1) show that 1 percent of congenital anomalies are caused by drugs, chemicals, and other exogenous agents (i.e., an estimated one in 400 infants has a birth defect with a teratogenic etiology). Estimates have not changed over several decades, perhaps because genomic research eclipses research in clinical teratology (Polifka and Friedman, 2002). Lack of research funding for research in human birth defects is often attributed to the higher priority given to genomic and other bench science. Little funding goes to birth defects monitoring or epidemiology. Much research remains to be done. The magnitude of the problem of medication use during pregnancy may be underestimated. Approximately 65–70 percent of birth defects have an unknown etiology, some of which may be unrecognized human teratogens not researched because of the lack of resources and funding. Unreported or under-studies of the teratogenic potential of medically prescribed medication contribute to our lack of information on many medications used in pregnancy.
Alcohol use and/or taking drugs of abuse, and other preventable causes of birth defects are likely under-ascertained. Congenital anomalies and other pregnancy complications caused by medication and chemical exposure are unique because these birth defects are potentially preventable. Key factors in evaluation and prevention of morbidity and mortality due to drug and chemical exposure during pregnancy include knowledge of prenatal exposure effects and the window of opportunity for intervention. Chapters 2–16 summarize information available regarding drug exposure during pregnancy. Drug-specific information obtained from the current medical literature, clinical experience, and science are reviewed for their potential to cause birth defects.
FIGURE 1.1 Causes of birth defects.
There is a narrow window of opportunity to intervene in medication use during pregnancy because pregnant women do not present for prenatal care until embryogenesis is complete (i.e., after 58 days post-conception). Intervention is further complicated because many women are not aware of the potential adverse effects of drugs and chemicals on pregnancy. For example, more than 60 percent of gravidas had never heard of fetal alcohol syndrome and were not aware of the adverse effects of alcohol on pregnancy in several surveys. The best intervention is patient education prior to conception; however, little to no funding is available for patient education. Social and cultural barriers must be effectively addressed for the patient education process to be successful.
Well-educated obstetrical patients use culturally based “folk etiologies” to explain the occurrence of birth defects and other adverse pregnancy outcomes. Folk etiologies rarely align medically founded causes. Even gravid physicians often incorrectly understand prenatal development and how medications and other environmental exposure can cause birth defects and other untoward pregnancy outcomes. Folk or sociocultural background and education level must be considered when counseling the obstetrical patient regarding specific drug and chemical exposure risks to pregnancy.
The good news is that the rate of birth defects has been reduced over time through avoiding teratogenic medications during pregnancy. The working hypothesis on reduction of congenital anomalies among women with epilepsy could be due to the increased adoption of dose adjustments during pregnancy to maintain an efficacious dose (Tomson et al., 2018). The not-so-good news is that research on drug use during pregnancy has not continued at the pace it could have because of funding and research priority (Adam et al., 2011; Lo and Friedman, 2002; Polifka and Friedman, 2002).
MAGNITUDE OF THE PROBLEM
The majority of women use a number of drugs during pregnancy, usually before they recognize they are pregnant. Medications are often related to a medical condition being treated before the pregnancy was known. Prevalence of medication use varies widely, <10 percent to more than 95 percent of pregnant women report drug use during gestation. Usually, more than one medication was used during pregnancy. A French study reported 89.9 percent of women used medication during pregnancy (Berard et al., 2019). In the United States, 97.1 percent of women used one medication during pregnancy, and 95.7 percent used medication during the first trimester (Haas et al., 2018). In a Danish study based upon blood samples, 82.6 percent of women used a drug during the first trimester (Aagaard et al., 2018). High prevalence of medication use during pregnancy is clearly a frequent event. Similar prevalences of drug use during pregnancy were reported in Brazil, Australia, New Zealand, and Egypt. Clearly, this is an international pattern and problem. Safety of drugs for use during gestation may be questionable or simply unknown in many instances (Polifka and Friedman, 2002). Paucity of clinical teratology research conducted over the last four decades is the root cause of poor availability of information on drug use in pregnancy (Lo and Friedman, 2002).
Inadvertent drug exposures during pregnancy are due to some medications being: (1) used before pregnancy is recognized, (2) taken without the physician’s advice after pregnancy is recognized, and (3) taken with a physician’s advice. In practice, the predominant case is that physicians are faced with determining whether or not a medication or drug may be harmful to a pregnant woman, or harm has been induced after the exposure has occurred.
Non-medical exposures to drugs are a concern in 10–20 percent of gravidas. Non-medical exposure to drugs during pregnancy occur in attempted suicide and substance abuse (i.e., recreational use). Suicide gestures in pregnancy occur in an estimated 0.6 percent. Substance abuse during pregnancy (discussed in Chapter 16) is >33-fold more prevalent than suicide gestures. An estimated 10–20 percent of pregnant women use an illicit or social substance of abuse. Cocaine seems to be the most frequently used substance in 2021.
CLINICAL EVALUATION
Clinical evaluation of drug exposure during pregnancy has five objectives that guide what is entered into the medical record and discussed with the patient (Box 1.1).
BOX 1.1 TERATOGEN EXPOSURE COUNSELING
Estimate date of conception.
Obtain the family history medical genetic pedigree.
Obtain information on the substances consumed (medications, alcohol, illicit/social substances of abuse), timing in gestation, frequency, and dose.
Integrate #1 and #3 to estimate exposure timing. Use the information from the calendar to determine the organ systems being formed during the exposure.
Compare the findings in #4 to the published literature and estimate the risk increase if there is one and it is known. If the results are reported in odds ratios, relative risks, or risk ratios, it is possible to ...