![]()
Techniques and Technical Issues
Chapter 1
Priftis KN, Anthracopoulos MB, Eber E, Koumbourlis AC, Wood RE (eds): Paediatric Bronchoscopy.
Prog Respir Res. Basel, Karger 2010, vol 38, pp 12–21
______________________
Bronchoscopic Equipment
Ian M. Balfour-Lynna · Jonny Harcourtb
aDepartment of Paediatric Respiratory Medicine, Royal Brompton Hospital, and bDepartment of Paediatric Otolaryngology, Chelsea and Westminster and Royal Brompton Hospitals, London, UK
______________________
Abstract
Bronchoscopic equipment is expensive and must be properly maintained. Sufficient initial outlay is required to provide adequate backup equipment. Modern hybrid bronchofibrevideoscopes combine digital technology with fibre-optic glass rods to produce an instrument that is small enough for use in children. These provide extremely clear images which can be digitally recorded and reproduced. A workstation is required to hold the ancillary equipment-flat-screen monitor, light source and video processor. Extra equipment is required for cleaning and disinfecting the bronchoscopes and their removable parts, and a proper storage space is necessary.
Copyright © 2010 S. Karger AG, Basel
Any hospital planning to set up a bronchoscopy service must be aware that this will require a significant start-up financial outlay. There will also be routine maintenance costs (e.g. cleaning, replacement of disposable parts) as well as occasional repair costs, which can be expensive if a bronchoscope is broken.
Flexible Bronchoscopes
It is important to have sufficient bronchoscopes to ensure that logistical problems are not encountered whilst servicing or repairs are being carried out. Occasionally a bronchoscope (or more usually its suction channel) malfunctions during a procedure itself, hence the need for a standby bronchoscope. Unfortunately some units may have difficulty with this due to the prohibitive price of bronchoscopes, which cost in the range of GBP 20,000.
There are several types of bronchoscopes available for paediatric use. Clearly the size of the bronchoscope used is dependent on the size of the airways (and hence the size of the child). In younger children, the smallest bronchoscope available should be used, in order to reduce blockage of the airway and minimize local trauma. The exception is if an endobronchial biopsy is to be performed, in which case it is better to use an instrument with the biggest available biopsy channel, provided that it is safe for the child [1]. The manufacturers usually describe the bronchoscope by the diameter of the distal tip; however, this is not always the maximum diameter of the bronchoscope. A small study has shown a discrepancy between the stated external diameter (of the tip) and the maximum diameter of the insertion tube that ranged from 0.19 to 0.66 mm, with a mean of 0.41 mm [2]. This is only likely to be relevant when a bronchoscope is used down an endotracheal tube (ETT) in a small child when the size is critical. In general, the larger the bronchoscope, the better the image obtained but even the smaller ones allow remarkably good views, with a 120-degree field of view. The image from the standard bronchofibrescopes is never as clear as that obtained by rigid bronchoscopes with their Hopkins rod lens telescopes. These are invariably the images found in textbooks, which can mislead trainees who need to be able to perform a bronchoscopy with suboptimal views. Since the advent of the hybrid bronchofibrevideo-scopes and bronchovideoscopes however, pictures can be as clear as those obtained with rigid bronchoscopes.
If the bronchoscope is being inserted down an ETT for general anaesthesia with assisted breathing, its size is critical as it partially blocks the ETT. This means a relatively smaller bronchoscope may need to be used for the size of the child, compared to inserting it via a laryngeal mask or down the nose via a facemask (table 1). The proportion of the cross-sectional area that the bronchoscope blocks can be calculated from this formula: [1 - (bronchoscope radius2/ ETT radius2) × 100]. Hence a 3.6-mm bronchoscope down a 5-mm ETT blocks 48% of the potential space for airflow. Generally the ETT internal diameter needs to be at least 1 mm greater than the external diameter of the bronchoscope [3; chapter 5, this vol., pp. 54-63].
Table 1. Sizes of flexible bronchoscopes that can be passed safely down differently sized ETTs, along with typical ages of relevant patients
| Bronchoscope external diameter | ETT internal diameter | Size of patient |
| 2.2 mm | 3.0- 3.5 mm | premature neonate |
| 2.8 mm | 4.0 mm | term neonate |
| 3.6 mm | 5.0 mm | small child (3-4 years) |
| 4.0 mm | 5.5 mm | child 4-8 years |
| 4.9 mm | 6.0 mm | child over 8 years |
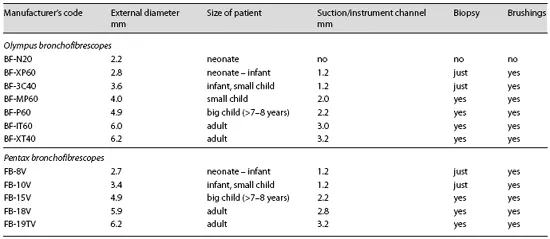
Table 2. Bronchofibrescopes
The smallest (Olympus) neonatal 2.2-mm bronchoscope has no suction channel, and its use has been limited since the advent of the 2.8-mm bronchoscope (with a 1.2-mm suction channel). Nevertheless, it may be used in a ventilated neonate with a 3-mm ETT in whom visualization of the airways is essential. The neonatal bronchoscope can only be used for a visual inspection, as lavage cannot be performed, but this can be hampered if mucus settles on the lens and obscures vision as it can usually not be cleared unless the whole scope is removed and wiped. In addition, the 2.2-mm bronchoscope is fragile and breaks easily.
The 1.2-mm suction/instrument channel is usually adequate for lavage and suction, the exception being when the secretions and mucus are excessively thick or sticky, as is typically found in children with more advanced cystic fibrosis lung disease. The larger 2-mm channel is also more useful when trying to suction up mucus plugs that have been blocking an airway. Excellent-quality biopsies can be obtained with 2-mm forceps that fit down the 2-mm working channel; reasonable biopsies can also be obtained from the smaller 1-mm forceps that fit the 1.2-mm channel but the procedure is more difficult and the biopsies are really quite small, hence often of poorer quality [4]. Lasers can be used in bronchoscopes with suction/ instrument channels of 2 mm and above, and ultrasonic probes in the 2.8-mm channel and above. These technologies are not usually employed in children [chapter 4, this vol., pp. 42-53].
Fig. 1. Bronchofibrescope with 3.6-mm outside diameter.
Table 3. Hybrid bronchofibrevideoscopes manufactured by Olympus
The principal manufacturers of paediatric bronchoscopes are Olympus and Pentax, and details of their available equipment are best seen on their respective websites (www. keymed.co.uk or www.olympusamerica.com; www.pentax.co.uk or www.pentaxmedical.com). Product information is accurate at the time of writing this chapter.
Bronchofibrescope
This is the classic fibre-optic bronchoscope (table 2, fig. 1) in which light and hence the image travels along extremely fine glass fibres (also known as image guide fibres or fibreoptic rods).
Hybrid Bronchofibrevideoscope
This has a built-in charge-coupled device in the control section and thus combines video and fibre-optic technology (table 3, fig. 2). This allows use of video technology in a smaller bronchoscope. The newer technology produces larger, clearer and brighter images, and there is an automatic focus and light adjustment. These scopes are also much lighter in weight and hence easier to handle.
Fig. 2. Hybrid bronchofibrevideoscope with 4.0-mm outside diameter.
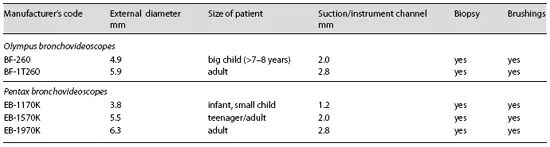
Bronchovideoscope
These are generally larger bronchoscopes (table 4) as the charge-coupled device is incorporated into the distal end of the instrument (‘chip in the tip’); they do not contain glass fibre rods.
Battery-Powered Bronchoscopes
Pentax make portable ‘bedside’ fibreoptic bronchoscopes (FB series) that run off a self-contained battery-powered light source. They can also be attached to a standard light source (table 5).
Intubation Bronchoscopes
Finally, Pentax make a series of fibreoptic intubation endoscopes for anaesthetists (FI series). The smallest is 2.4 mm but has no suction channel.
Table 4. Bronchovideoscopes
Table 5. Battery-powered bronchoscopes manufactured by Pentax
Hence to take advantage of the better images obtained by digital video technology, paediatricians will need to use the Olympus hybrid 2.8- and 4.0-mm bronchoscopes, or the Pentax 3.7- and 5.1-mm bronchoscopes.
Bronchoscope Components
The bronchoscope attaches to the light source and video processor from a fixed lead that comes off the control section (proximal part of bronchoscope). The eyepiece (on bronchofibrescopes) is at the tip of this part, and when attached to a TV monitor an attachment locks onto the eyepiece with a bayonet mount. A manual focus button is on this attachment as well as remote control buttons that can be used to control video recording and still pictures. Hybrid and videoscopes do not require this attachment, and the buttons to control recording are just distal to the suction valve; focus is automatic, so there is no separate control button.
The suction valve is sited on the control section (convenient for the index finger) but can be taken off to be autoclaved. Stand-alone suction pumps (or wall suction) connect to the valve with disposable suction tubing.
Lower down this section is the biopsy port, through which lavage fluid, biopsy forceps and brushes are inserted.
The control section also has the lever (convenient for the thumb) which controls the distal tip of the bronchoscope; this allows a bending angle upwards of 180° and downwards of 130°. The Pentax K series (3.7 and 5.1 mm) bronchosc...