![]()
Chapter 1
Domanski HA, Walther CS: FNA Cytology of Soft Tissue and Bone Tumors. Monogr Clin Cytol.
Basel, Karger, 2017, vol 22, pp 1–12 (DOI: 10.1159/000475088)
___________________
Principles in the Examination and Management of Soft Tissue Lesions
Clinical Features and Team Work
Soft tissue neoplasms comprise a heterogeneous group of lesions with mesenchymal differentiation. Sarcomas are rare, constituting less than 1% of all malignant neoplasms. Benign soft tissue tumors are estimated to be approximately 100 times more frequent than sarcomas. Soft tissue tumors may occur in different planes and locations. However, 99% of benign soft tissue tumors are superficial while two-thirds of the extremity and trunk-wall sarcomas are deep seated. Age-specific incidence rates clearly demonstrate that soft tissue sarcomas are more common with increasing age. There is a slight male predominance, but the gender- as well as age-related incidence is also related to the histologic type and subtype of sarcomas.
In the course of the diagnostic workup of soft tissue masses, a biopsy is necessary in most cases to confirm malignancy and in the case of sarcoma to assess the grade of malignancy and the histologic type. The difficulties in diagnosing patients with musculoskeletal tumors stem mainly from their rarity and to the lack of experience with the microscopic appearance of soft tissue lesions on the part of most pathologists not working in orthopedic-oncology centers [1, 2].
The best approach to a successful diagnostic evaluation of musculoskeletal lesions is to combine clinical data and radiographic findings with the morphologic interpretation of cells and tissue, complemented by ancillary techniques. In specialized orthopedic-oncology centers, orthopedic-surgical, oncologic, radiologic, pathologic/cytologic, and molecular biologic expertise can be combined in a multidisciplinary team to allow the adequate evaluation and therapy, as well as follow-up, of patients with musculoskeletal neoplasms. This multidisciplinary management of musculoskeletal neoplasms favorably influences outcomes for patients suffering from sarcoma [3–7].
Biopsy Techniques
Tumor tissue sampling is necessary for the diagnosis of soft tissue tumors in which malignancy cannot be ruled out by clinical or radiographic means. Open incisional and excisional (local excision for small and superficial lesions) biopsy and core-needle biopsy (CNB) are generally accepted as sampling techniques in the diagnosis of musculoskeletal neoplasms [8]. Open biopsy usually provides sufficient tissue for histopathologic examination as well as for ancillary studies. However, there are risks of intraoperative and postoperative complications and occasional delays in therapy initiation while the surgical wound heals. In addition, incisional biopsy can break natural barriers to tumor growth, which can adversely affect subsequent surgical procedures and increase the risk of the spread of the tumor into surrounding tissues. CNB has become a popular diagnostic procedure since it can be performed in an outpatient setting and carries a very low risk of morbidity. The evaluation of CNB specimens may be challenging due to limited sampling and the heterogeneity of most soft tissue neoplasms.
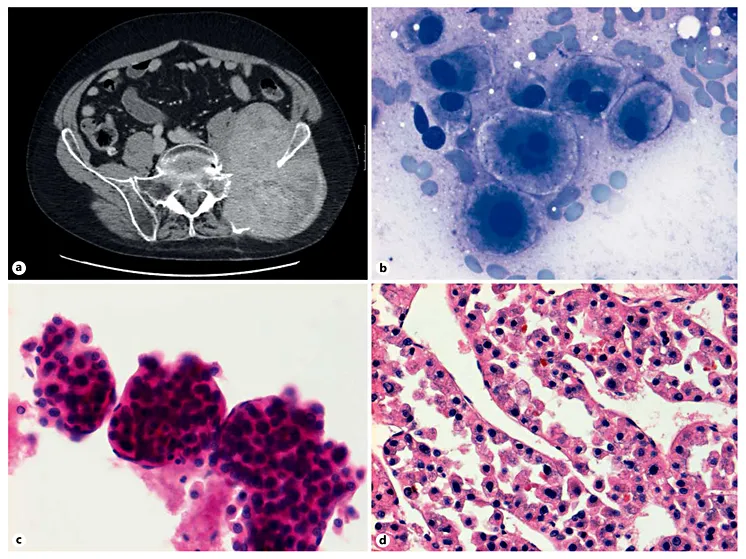
Fig. 1. a MRI with a large pelvic mass extending to the gluteal soft tissue. Clinically suspicious of sarcoma. b FNAC of the gluteal mass showing large tumor cells with rounded nuclei and abundant finely granulated cytoplasm, resembling hepatocytes. Binucleated and multinucleated tumor cells. MGG stain. c Thick clusters of tumor cells with endothelial wrapping, features of hepatocellular carcinoma. HE stain. d Cell block confirms the diagnosis metastasis of hepatocellular carcinoma. HE stain.
An increasing use of minimally invasive diagnostic procedures has resulted in better acceptance of fine-needle aspiration cytology (FNAC) as a first-line approach or as a complementary tool to CNB in the diagnosis of musculoskeletal lesions [9, 10, 11]. An FNAC diagnosis is generally accepted in the evaluation of suspected recurrences or metastases of soft tissue neoplasms, as well as in the diagnosis of metastatic carcinoma, melanoma, or lymphoma presenting clinically as primary soft tissue neoplasms (Fig. 1). The accuracy of FNAC in distinguishing benign from malignant soft tissue tumors and sarcoma from other malignancies has been shown to be comparable to that of surgical biopsies, while its accuracy in the grading of soft tissue sarcoma and in establishing a specific histologic diagnosis has been shown to be inferior to both CNB and surgical biopsies. The accumulated experience from centers with expertise in the cytologic examination of musculoskeletal lesions has established additional major indications for FNAC, such as the diagnosis of primary benign/locally aggressive soft tissue tumors and soft tissue sarcomas [7, 9, 11, 12]. The role of FNAC in the initial diagnosis of primary soft tissue is still debated, however, and the current literature has not completely clarified the optimal biopsy technique for the diagnosis of soft tissue tumors [8, 11, 13–15].
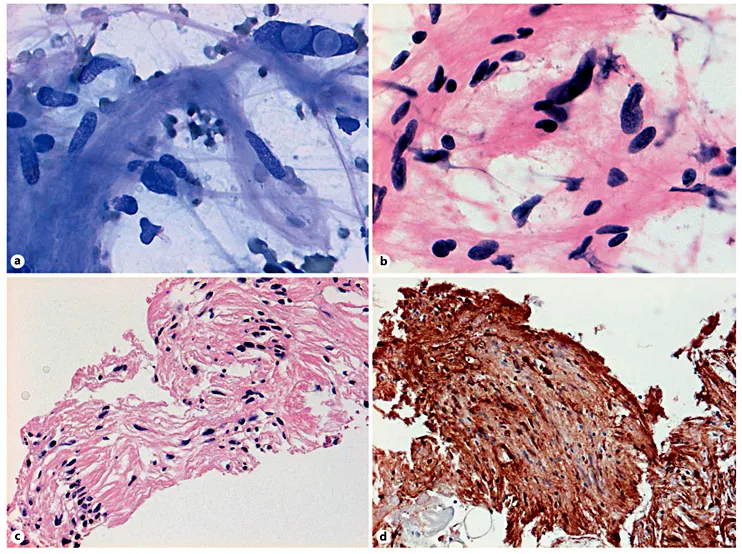
Fig. 2. a ROSE: FNAC of the soft tissue mass in the thigh showing a loosely cohesive cluster of atypical spindle cells. Note the tumor cells with intranuclear inclusions and the fibrillary background of the smears, which are features suggestive of ancient schwannoma. DiffQuick stain. After rapid examination of the first smear, additional passes of FNA were performed in order to obtain more material for ancillary studies. b Alcohol-fixed smears showing a loosely cohesive cluster of spindle cells with anisokaryosis and hyperchromasia worrisome for malignancy. HE stain. c Cell block showing palisading spindle cells creating a Verocay body and architectural patterns consistent with schwannoma. HE stain. d Strong and diffuse positivity for S100 on a cell block section confirms the diagnosis of ancient schwannoma.
Advances and Limitations of Fine-Needle Aspiration Cytology in the Diagnosis of Soft Tissue Neoplasm
Compared to open biopsy, FNAC has some advantages and also some limitations [2]. Among its advantages, FNAC is an outpatient procedure which is well tolerated by patients and has negligible risks for serious complications. With thin needles, it is easy to sample material from different parts of large tumors, thereby revealing possible tumor heterogeneity. While tumor tissue architecture is better evaluated in surgical biopsies, it can also be evaluated in cell blocks prepared from specimens obtained by FNA (Fig. 2). Through rapid staining applied to aspiration smears, the FNA technique allows for the immediate evaluation of specimen adequacy while the patient waits, known as “rapid on-site evaluation” (ROSE) [16–18]. If necessary, additional aspirations and CNB can be performed in order to obtain material sufficient for microscopic examination and for ancillary studies (Fig. 2).
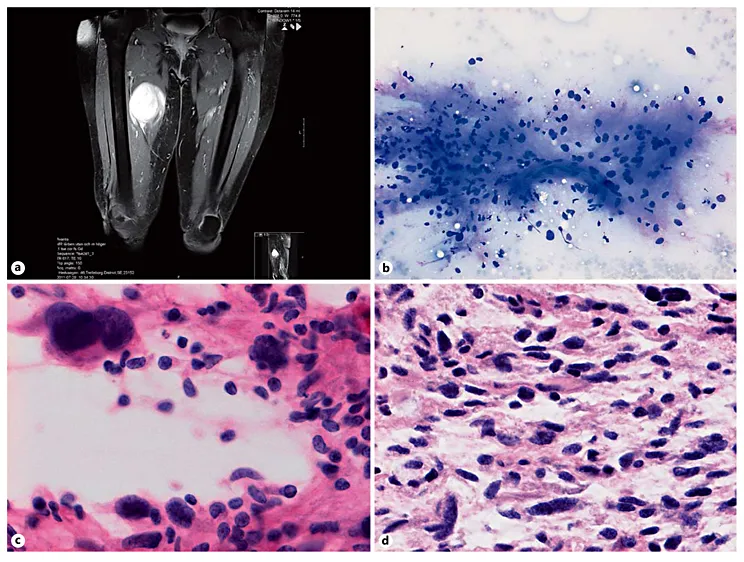
Fig. 3. a MRI showing a deep soft tissue mass in the right thigh suspicious for soft tissue sarcoma. b FNAC of the mass shows a loosely cohesive cluster of atypical epithelioid and spindle cells and a capillary vessel fragment embedded in a fibromyxoid matrix, which are cytologic features suggestive of myxofibrosarcoma. MGG stain. Alcohol-fixed smears (c) and the cell block section (d) show moderate to severe nuclear atypia of tumor cells suggestive of a high grade of malignancy. HE stain.
Generally, the cytomorphology of single cells, in technically satisfactory smears, is superior to that seen in core-needle and open biopsy specimens. The FNA procedure requires fewer resources than other biopsy techniques and is the most cost effective. In addition, the technique of FNA is both easy to perform and easy to learn.
The main disadvantage of FNAC, however, is that samples are very small and it can be difficult to obtain sufficient material for both morphologic examination and all necessary ancillary studies. In addition, there is a lack of pathologists/cytopathologists experienced in the cytologic evaluation of soft tissue lesions.
Fine-Needle Aspiration Cytology according to the WHO Classification
Nomenclature and the classification of soft tissue neoplasms used in daily clinical practice are based on the WHO classification of soft tissue and bone neoplasms. During the workup of patients with soft tissue tumors, every effort should be made to establish a histologic diagnosis according to the WHO classification and, in the case of sarcoma, the histologic grade of the neoplasm. A histologic diagnosis of soft tissue yield can occasionally be difficult to establish using routine cytologic smears alone. The aspiration of material sufficient for cell blocks and for ancillary techniques is an important part of the cytologic examination and can require ROSE of the yield. In addition, cytologic examination is an easy and quick method to establish or exclude malignancy, exclude carcinoma, melanoma or lymphoma, and can guide the subsequent diagnostic workup. (Fig. 1–3).
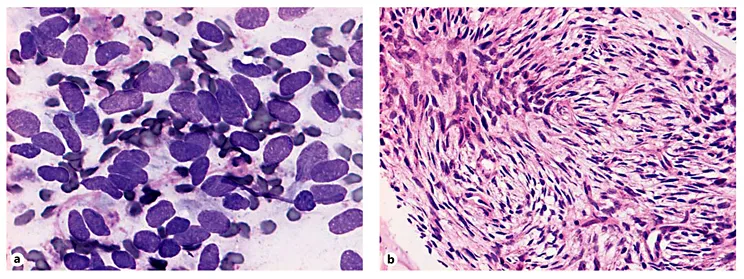
Fig. 4. a The sarcoma grade of malignancy may be determined by the histologic dia...