
The Hands-on Guide to Diabetes Care in Hospital
David Levy
- English
- ePUB (handyfreundlich)
- Über iOS und Android verfügbar
The Hands-on Guide to Diabetes Care in Hospital
David Levy
Über dieses Buch
3 am call: 'Mrs X has a blood sugar of 23. Come and deal with it'
'I think my insulin pen is called something like Solostar'
The respiratory doctors started high dose prednisolone, and the patient's glucose is 18
'What is the blood glucose target for this patient admitted with an acute coronary syndrome?'
Do you struggle with common diabetes problems in hospital practice? The Hands-on Guide to Diabetes Care in Hospital is an ideal companion for ward practitioners, providing answers to these and many other practical diabetes problems, helping you to deliver safe and effective care to patients.
Using the best current UK and international guidance, The Hands-on Guide to Diabetes Care in Hospital presents succinct guidance on acute diabetes problems, blood glucose management, acute medical and surgical problems commonly complicated by diabetes and insulin and non-insulin agents, as well as preparing for discharge to the community. With top tips, key points, questions to ask, treatment and follow-up advice in each chapter, this is an essential resource for all medical trainees and students who treat diabetic patients. Ward-based nurses, diabetes specialist nurses and pharmacists will also find a lot that is relevant to their practice.
Take the stress out of diabetes care with The Hands-On Guide!
www.wiley.com/go/handsonguides
Häufig gestellte Fragen
Information
PART 1 Basics
1
Classification of diabetes
Key points
- Diabetes is either Type 1 or Type 2. No other terms for these major categories are permitted
- The formal diagnosis is not always obvious in acutely admitted patients (either newly diagnosed or not previously fully characterised)
- Apart from patients with DKA, you will not encounter Type 1 patients very often; this makes it especially important to identify them, as their management is completely different from that of most Type 2 patients
- Among the other specific types of diabetes (of which there are many, mostly rare), two concern the acute hospital practitioner:
- Pancreatic
- Drug-induced
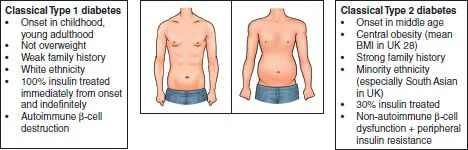
Phenotypic features of classical Type 1 and Type 2 diabetes
- Someone on full insulin treatment alone (a regimen that covers night-time and meal times without non-insulin agents) is probably Type 1
- Exception: some patients with very long duration Type 2 diabetes (often thin, with pancreatic 2018;exhaustion’) take only insulin
- Most Type 2 patients on full insulin usually take metformin as well (they may also take injectable GLP-1 analogues and a variety of oral agents; see Chapter 24)
- Someone on full insulin since childhood, adolescence, or early adulthood (up to 30–35) is Type 1. Most patients can remember accurately how long they have been taking insulin. Late-onset Type 1 diabetes can occur at any age (often in people with a strong personal or family history of associated autoimmune conditions)
- Northern Europe (especially UK and Scandinavia), Australia and New Zealand have the highest incidence of Type 1 diabetes
- A non-overweight white person of any age treated with insulin alone has Type 1 diabetes. Many people now survive without significant complications for 50 years or more (they will be in their 60s and 70s). They often need only tiny doses of insulin (e.g. <20 units/day) but are still insulin-requiring and ketosis-prone
- Thin people are likely to have Type 1 diabetes, but there are a lot of overweight Type 1 patients who have insulin-resistant features and may require high-dose insulin
Terminology
| Type 1 | Type 2 | Comments |
| Type I | Type II | Use Arabic, not Roman numerals, National Diabetes Data Group (NDDG), 2003 |
| Insulin-dependent | Non-insulin-dependent | Declared obsolete, 2003 (NDDG) |
| IDDM | NIDDM | Declared obsolete, 2003 (NDDG). It’s hazardous to use ... |