Giuseppe Micali, Francesco Lacarrubba, Giuseppe Micali, Francesco Lacarrubba
This is a test
This is a test
208 páginas
English
ePUB (apto para móviles)
Disponible en iOS y Android
eBook - ePub
Dermatoscopy in Clinical Practice
Beyond Pigmented Lesions
Giuseppe Micali, Francesco Lacarrubba, Giuseppe Micali, Francesco Lacarrubba
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Dermatoscopy has been heavily promoted to dermatologists as the front line in detecting skin cancer early and easily. However, this technology also has other uses in everyday dermatologic practice.
Dermatoscopy in Clinical Practice shows those already using the equipment how they can extend its use beyond pigmented lesions and exploit its full potential. Dermatoscopy and videodermatoscopy can be used for differential diagnosis, prognostic evaluation, and monitoring response to treatment of various disorders including inflammatory diseases, parasitoses, viral and fungal infections, nonpigmented skin lesions, hair abnormalities, and a large variety of other dermatologic conditions as well as cosmetology.
The book focuses on those conditions in which the techniques are most useful, describing the clinical and histopathological correlations associated with the procedure. The book includes color clinical images throughout, making it a handy guide for the dermatologist's daily practice.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
Simplemente, dirígete a la sección ajustes de la cuenta y haz clic en «Cancelar suscripción». Así de sencillo. Después de cancelar tu suscripción, esta permanecerá activa el tiempo restante que hayas pagado. Obtén más información aquí.
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Dermatoscopy in Clinical Practice un PDF/ePUB en línea?
Sí, puedes acceder a Dermatoscopy in Clinical Practice de Giuseppe Micali, Francesco Lacarrubba, Giuseppe Micali, Francesco Lacarrubba en formato PDF o ePUB, así como a otros libros populares de Medicine y Medical Theory, Practice & Reference. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Pietro Rubegni, Niccolò Nami, Luca Feci, Marco Burroni, Linda Tognetti, and Michele Fimiani
DERMATOSCOPY
The optical dermatoscope is an instrument containing a light source that enables skin structures invisible to the naked eye to be seen. A medium such as ultrasound gel or vaseline oil is applied to the skin to make the stratum corneum transparent (epiluminescence technique), and the dermatoscope lens is placed against the skin surface. The instrument makes it possible to observe a vast new range of dermatological signs. A limitation of the handheld dermatoscope is represented by maximum ×10 magnification. In addition, many devices do not allow image storage, although new models can be connected to photocameras or smartphones for storage and post-processing.
Dermatoscopy is currently used in routine dermatology. The various specialist courses held in recent years have led to the definition of new methods for improving the diagnosis of neoplastic and other skin disorders.
VIDEODERMATOSCOPY
ANALOG VIDEODERMATOSCOPY
Between 1980 and 1990, advances in video technology led to the development of instruments that displayed dermatoscopic images on a screen.1 The first videodermatoscopes had a telecamera with video resolution connected to an optical dermatoscope and a television screen with video recorders to record examinations. They suffered from low quality due to the low resolution of the first video cameras and cumbersome documentation and data-saving procedures. Maximum television resolution is 768 × 576 pixel for the European PAL Broadcast system and less for the US National Television Systems Committee (NTSC) where pixel is the basic image unit; analog video recorders of the 1980s often had less than 400 horizontal lines. Low quality and technical limitations prevented the widespread use of videodermatoscopy.2
DIGITAL VIDEODERMATOSCOPY
Between 1990 and 2000, computerized instruments for digitizing images from telecameras connected to videodermatoscopes became common. Digital dermatoscopic images can be obtained by conversion from video-telecameras connected to digital cards or by use of high-resolution digital telecameras or digital cameras coupled with special dermatoscopy adaptors. Computerized systems proved more practical for managing examinations because they offered the possibility of saving personal and private data of patients together with digital images of pigmented skin lesions (Figure 1.1).2–3
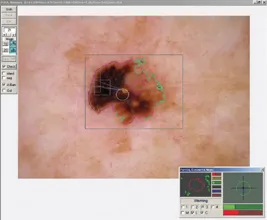
In the case of video-telecameras, the signal acquisition peripheral required a charge coupled device (3CCD) or sensor for the red, green, and blue bands, to keep image quality high during sampling.1,4 Digital telecameras have better quality for the equivalent video characteristics because they do not require any conversion. They can have a USB (usually amateur grade) or Firewire (professional grade faster and better quality) interface. Much higher resolution is possible with digital telecameras than with analog video telecameras, and this has clear diagnostic advantages, as digital dermatoscopy systems of this type can reach 1280 × 1024 pixel with images observed in vivo at 15–25 photograms per second on computer screens (Figure 1.2). Digital cameras provide exceptionally high resolutions (up to 3000 × 2000 are common) but have the disadvantage of not providing full-resolution images in vivo but only after the images have been saved.
FIGURE 1.1 Digital videodermatoscope.
Figure 1.2 “Real-time” digital dermatoscopy analyzer.
The two types of digital instruments are therefore designed for different users. Clinicians who use video or digital telecameras (usually specialist centers) perform many examinations to diagnose melanoma or inflammatory skin diseases and observe many lesions by digital technology. Digital cameras are largely used to document lesions first observed by traditional dermatoscopy.5
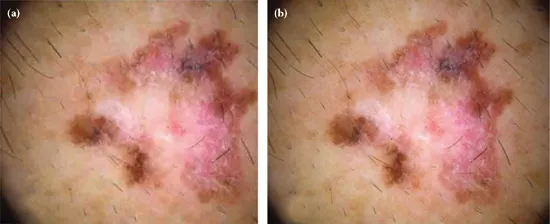
It is commonly thought that a higher number of pixels implies better quality images; this is untrue, even if resolution is the imaging system’s ability to reproduce details. Image quality is determinant for early diagnosis of melanoma and depends on factors such as the optical system of the instrument, illumination, type of instrument, and resolution.6 Digital dermatoscopy images generally have between 768 × 576 and 1600 × 1200 pixel; lower resolution compromises diagnosis and higher resolution is unnecessary (Figure 1.3). The definition of magnification is only valid for integrated instruments with the same screens. Field of view is a preferable parameter. Dermatoscopy optical systems generally enable a horizontal field of view between 2 mm and 3 cm to be viewed. Overall magnification M of digital dermatoscopes is calculated as the ratio of screen diagonal D to field of view diagonal d: M = D/d.
Illumination must be homogeneous and sufficiently strong, while incident intensity should be modified by the lens diaphragm rather than by varying electrical potential, to keep the color of the study area constant. Reddish or saturated images result from low-quality equipment or failure to balance white chromatic calibration.
FIGURE 1.3 (a) Dermatoscopic image at 512 × 384 pixel resolution (42.8 KB). (b) The same image at 1024 × 768 pixel resolution (326 KB).
On the basis of the observation that in adult patients benign lesions remain stable whereas melanoma tends to grow and change over time, digital follow-up of melanocytic lesions has been proposed as a strategy to recognize melanoma. Stratification of the risk of developing melanoma is of great importance to establish the best strategies and follow-up methods. The intervals between successive dermatoscopy examinations vary. Most frequently the first checkup is performed 3 months after initial examination; further follow-up is performed every 12 months. Short-term follow-up is oriented toward assessment of single melanocytic lesions, while medium (every 6 months) and long-term (every 12 months) follow-up is focused on monitoring of multiple lesions. The lesions selected for short-term follow-up usually fall into two categories: moderately atypical lesions without a history of change and mildly atypical nevi with a history of change. Long-term follow-up is used for the surveillance of patients with atypical mole syndrome or high nevi count, among other risk factors. Short-term follow-up (after 3 months) may be the only way to recognize early melanoma.7–8
CONTACT, NONCONTACT, AND POLARIZED DERMATOSCOPY
Today there are many types of dermatoscopes. Contact incident-light dermatoscopes use a glass window placed in contact with the skin, illuminated at an angle of about 30–45 degrees so as to eliminate direct reflection, and a magnifying lens system.9 A liquid fills the space between the skin and the glass, rendering the skin translucent and revealing subcutaneous patterns invisible to the naked eye.9–11
Two polarizing filters can be added to this simple optical system, one before the telecamera sensor and one on the light source, to eliminate light reflected by cross-polarization. Light reflected from the skin surface maintaining the polarization of the light source is eliminated by the polarizer in front of the sensor; this enables skin patterns to be observed to a greater depth. Pol...