In Our Clients' Shoes conveniently assembles a number of important papers on the Therapeutic Assessment approach in one resource, explicating its history, theory, techniques, as well as its impact on clients and assessors. Author Stephen E. Finn incorporates pieces presented at various conferences over the past 13 years, in addition to previously unpublished work, with the intent to allow psychologists greater insight into their clients' perspectives.
Arranged in three sections, the first set of papers describes the history and development of Therapeutic Assessment, including personal experiences of the author, which ultimately led him to focus on psychological assessment as a potential therapeutic intervention. The second section follows with a variety of essays to illustrate particular techniques of collaborative and Therapeutic Assessment. In this section, readers gain an understanding of how to integrate test findings, engage clients in discussing their experiences of a test, conduct assessment intervention sessions, and teach Therapeutic Assessment to graduate students. Finn concludes by drawing a link between Therapeutic Assessment and two major schools of psychotherapy: intersubjectivity theory and control-mastery theory. He also discusses how assessors grow and change as a result of practicing psychological assessment, and addresses practical matters such as when to apply the approach, how to bill for Therapeutic Assessment sessions, how to market Therapeutic Assessment, and where to find professional support for this kind of work.
In Our Clients' Shoes is appropriate for all clinicians who wish to further impact the lives of their clients and enhance their own wisdom, compassion, and personal and professional development.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
Simplemente, dirígete a la sección ajustes de la cuenta y haz clic en «Cancelar suscripción». Así de sencillo. Después de cancelar tu suscripción, esta permanecerá activa el tiempo restante que hayas pagado. Obtén más información aquí.
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es In Our Clients' Shoes un PDF/ePUB en línea?
Sí, puedes acceder a In Our Clients' Shoes de Stephen E. Finn en formato PDF o ePUB, así como a otros libros populares de Psicologia y Storia e teoria della psicologia. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Part I The History and Development of Therapeutic Assessment
1 Introduction: What Is Therapeutic Assessment?
Definitions and Distinctions
As Therapeutic Assessment has become more accepted in recent years, people are starting to use this and related terms in different ways. For this reason, I find it useful to define my terms and make certain conceptual and practical distinctions. I do this humbly—realizing that my definitions may be different from those of other people who think, write, and practice in this area, and that the distinctions I make are “fuzzy” and do not map precisely onto real life.
Traditional Assessment
In 1997, Mary Tonsager and I published a paper in which we contrasted traditional “information-gathering” psychological assessment and Therapeutic Assessment on a number of dimensions (Finn & Tonsager, 1997). That detailed analysis is still useful, but for my purposes here let me simply define traditional assessment as that model where psychological tests are administered to clients primarily for the purposes of diagnosis, treatment planning, treatment evaluation, and/or increased understanding. The main emphasis in traditional assessment is typically on the standard- ized data that is carefully collected by the “expert” assessor (or an assistant), who then compares test scores to nomothetic norms in order to derive conclusions that will be useful in understanding, communicating about, and treating a certain “patient,” or in monitoring the progress of treatment.
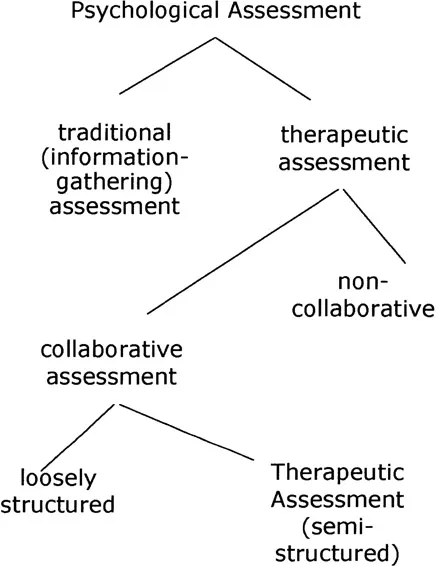
EXHIBIT 1-1 Types of Psychological Assessment
“therapeutic assessment”
Next, let me define therapeutic assessment (lowercase). Mainly, I consider this to be an attitude about psychological assessment—where the goal of the assessor is more than collecting information that will be useful in understanding and treating the patient. In therapeutic assessment, in addition, assessors hope to make the assessment experience a positive one and to help create positive changes in patients and in those individuals who have a stake in their lives (such as family, therapists, and employers).
Therapeutic assessment is based on the intent to use psychological assessment to help patients directly, rather than just indirectly, as with traditional assessment. Apart from this intent, from my observations, therapeutic assessment is not tied to any particular set of procedures, clinical techniques, or philosophy. It is practiced in a variety of ways, and I further believe that many clinicians are conducting therapeutic assessments without even claiming to do so! An example of a gifted psychologist who positively impacted clients through his assessments—without ever asserting that they were explicitly therapeutic—was Paul Lerner (2005a, 2005b).
Collaborative Assessment
I also find it useful to distinguish between collaborative and noncollaborative therapeutic assessment. One thing probably common to all therapeutic assessment is that assessors generally have some thoughtful way that they communicate information derived from an assessment directly to patients. In my mind, collaborative assessment goes beyond the practice of giving feedback, even if that is done in an interactive way. It involves a comprehensive effort to engage the client in multiple phases of the assessment process—including (a) framing the reasons for the assessment, (b) observing test responses and behaviors, (c) discovering the significance of those responses and behaviors, (d) coming up with useful recommendations, and (e) drafting summary documents at the end.
Collaborative psychological assessment is probably almost always beneficial to clients, and as such I consider it a subset of therapeutic assessment. But collaborative assessment may not always start with the explicit intent to produce positive change. For example, three pioneers of collaborative assessment—Connie Fischer (1985/1994), Len Handler (1995), and Caroline Purves (1997)—were all practicing collaborative assessment for years before they openly acknowledged that their assessments were therapeutic to clients. All three developed their approaches by trying to make the assessment process more humane, respectful, and understandable to clients, or, as Fischer (1985/1994) wrote, by gradually eliminating those aspects of psychological assessment that were dehumanizing or potentially harmful to clients.
Fischer also articulated a coherent philosophy of science, based in phenomenological psychology, which grounds and extends collaborative assessment techniques. My brief summary of this intersubjective model is as follows: “We can never know some external reality in its own right. We inevitably participate in what we see, always using our perspectives, backgrounds, and interests to assign meaning to our observations.” (See chap. 17 for a more extensive discussion of Fischer’s theory.) This point of view establishes an attitude about psychological test scores and their relationship to real-life events that permeates many aspects of collaborative assessment. If you grasp and believe Fischer’s model, you will never, for example, find yourself arguing with a client over the meaning of a test score (e.g., “What do you mean, you aren’t depressed? Your MMPI-2 Scale 2 score is 98!”). Also you will be intrigued, naturally, about the client’s own thoughts about that MMPI-2 score and the match between what psychologists call “depression” and that client’s own experiences. If you believe in phenomenological psychology, no one will have to tell you to discuss these matters with the client; you will just do so! For these reasons, I believe that Fischer’s human—science framework encourages greater consistency in and expansion of collaborative assessment techniques, and it therefore underlies much of my own work on Therapeutic Assessment, to which I now turn.
Therapeutic Assessment
I reserve the term Therapeutic Assessment (uppercase) for the semistructured collaborative assessment approach—grounded in Fischer’s human—science philosophy—that has been developed by me and my colleagues at the Center for Therapeutic Assessment in Austin, Texas. I call Fischer’s, Handler’s, and Purves’s approaches “loosely structured” collaborative assessment because there is a systematic method to their work—but it’s not spelled out as explicitly as in Therapeutic Assessment. I do not claim that our method produces greater benefits to clients than the less structured forms of collaborative or therapeutic (lowercase t) assessment. However, I do believe it is somewhat easier to teach and to research and that its organization helps guide assessors through the many complex choice points that arise in a collaborative assessment. I’ve often said—and I’m only half jesting—that Therapeutic Assessment is for those of us who are not as creative, intuitive, and quick on our feet as are Fischer, Handler, and Purves. If you follow the structure of Therapeutic Assessment for a period of time, gradually you will know when it is appropriate to deviate from this format and feel confident doing so. I’m reminded of the promise of my childhood piano teacher, who told me that if I practiced my scales diligently, someday I would be able to play jazz. Recently I see the truth of this statement in the assessments I do with my clients.
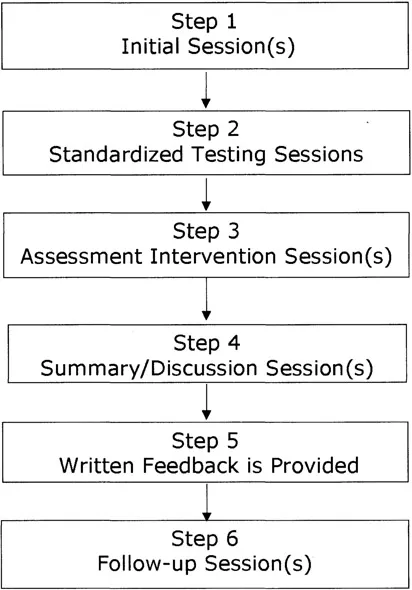
EXHIBIT 1–2 General Flow Chart of a Therapeutic Assessment
Flow Chart and Brief History of Therapeutic Assessment
So let me review the general structure of a Therapeutic Assessment, explaining, as I proceed, how the different steps developed and were incorporated into the model. Thus, rather than presenting the steps in the order they appear in an assessment, I discuss them in the order in which they found their way into Therapeutic Assessment.
Step 4—Summary andlor Discussion Sessions
I first became convinced of the potential therapeutic value of psychological assessment during my graduate training. During this period, I had several moving and powerful experiences discussing assessment results with clients, and they reported afterwards that their lives were changed. (I relate some of these experiences in chap. 2.) Not surprisingly then, as I became interested in understanding how assessment could be therapeutic and in discovering ways to make it more so, I initially focused on what I then called “feedback sessions” with clients.
One of the things I explored in my early research concerned how to order the information we present in feedback sessions to make those sessions the most useful and beneficial to clients. At first, most clinicians I consulted suggested that one should start by telling clients something positive about themselves. It turns out that this is not always the best practice, especially with clients who have very negative self-images. Instead, my colleague Bill Swann and I demonstrated (Schroeder, Hahn, Finn, & Swann, 1993) that clients are most able to integrate and make use of assessment information when it is presented in the following order:
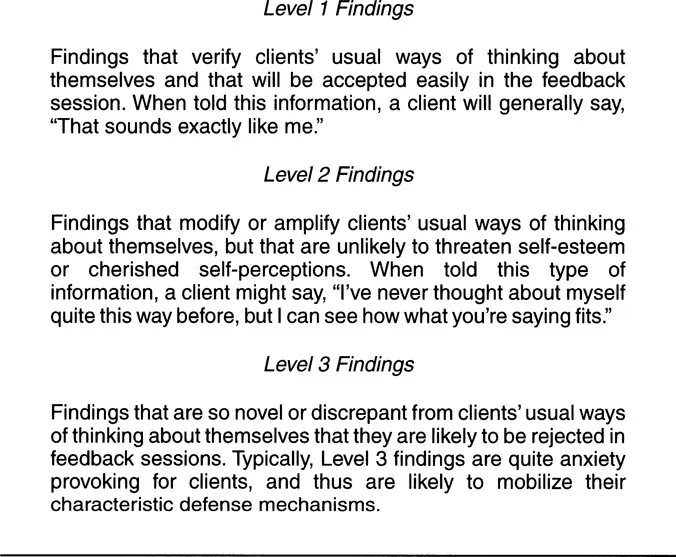
(1) Begin with what I call Level 1 findings—those that map onto the way clients already think about themselves. An example would be telling a self-labeled extrovert that his very low score on Scale 0 of the MMPI—2 suggests that he enjoys meeting new people, is comfortable in large groups, and would not do well in a job where he worked mainly on his own.
(2) Next, introduce Level 2 findings from the assessment, which reframe or amplify clients’ usual ways of thinking about themselves. This might involve telling a client who is concerned about lethargy, lack of motivation, and poor focus, that his Rorschach D score of −4 suggests he is emotionally overwhelmed, rather than just “lazy” as he fears.
(3) Last, if all is still going well, you may introduce Level 3 findings to clients—those that conflict in some major way with their usual conceptions of themselves. Research has shown that in many instances clients continue to consider and assimilate such information long after an assessment is completed.
EXHIBIT 1–3 Ordering Resuts Presented to Clints from a Psychological Assessment
Besides collaborating with me on the research that supported this way of discussing assessment results with clients, Swann’s own work helped provide an explanation for why this approach works best (Swann, 1996, 1997; Swann, Stein-Seroussi, & Giesler, 1992). His self-verification theory posits that people have a drive to maintain the current “stories” or “schemas” they have about themselves and will often discount or push aside information that conflicts with these stories. This is true even if a person’s existing self-story is primarily negative, as anybody knows who has tried to pay a compliment to a person with low self-esteem (Swann, Wenzlaff, Krull, & Pelham, 1992). By starting an assessment feedback session with self-verifying information and gradually moving to findings that are less self-verifying, one creates the optimal condition for clients to incorporate new information into the ways they think about themselves and the world.
Once I understood self-verification theory, I began to clarify the most appropriate focus of intervention in a psychological assessment—that is, clients’ existing conceptualizations of themselves and other people. I realized that if we could assist clients in changing these stories—which often are vague, inaccurate, and lacking in self-compassion—we could profoundly impact their lives. Around this time, I also had two other insights about feedback sessions. First, I knew that people do not change their beliefs about themselves easily, and that I would need to support people emotionally—in a tangible way—to help them assimilate and accommodate to new information. This spurred me to work on and improve my ability to mirror and connect with clients deeply in a short period of time. Second, experience told me that I could best help clients change their stories by dialoguing with them about the assessment findings and explicitly asking them to agree, disagree, revise, and give real-life examples of what I was saying. Research by Hanson and others has since confirmed that this interactive style of discussing assessment results benefits clients more than a unilateral, assessor-driven presentation of test findings (e.g., Hanson, Claiborn, & Kerr, 1997). For this reason, I no longer talk about conducting “Feedback Sessions” at the end of an assessment, preferring now to call them “Summary/Discussion Sessions.”
Step 1—Initial Sessions
The next set of developments in Therapeutic Assessment concerned initial sessions. In listening to clients who voluntarily agreed to participate in psychological assessments, I realized that certain aspects of their self-schemas were more open to change than others. And sometimes, clients themselves were actively searching for new ways of thinking about themselves and the world. This led to the practice of asking clients—in the initial assessment sessions—what puzzles, questions, or quandaries they had about themselves, and then making these questions the focus of the assessment. My initial thought was that such questions would signal me where clients’ stories were most flexible, serving as “open doors” through which one could send assessment information during the feedback session. This proved to be true, and my colleagues and I found that Level-3 findings were much more likely to be accepted by clients if they could be related to the clients’ own puzzles about themselves. Also, clients’ assessment questions often revealed a lot of information about their existing self-schemas, and one could often discover what was Level-1 information by asking clients in the initial session for their best guesses—before any testing was done—about the answers to their questions. Finally, by focusing psychological assessments on clients’ personal agendas, we made the whole assessment process much more client-centered, which seemed to lower clients’ anxiety, enlist them in the assessment in an active way, and engage their curiosity.
All of these factors seemed to enhance the therapeutic impact of our assessments, but as time has gone on I have become more convinced of the value of helping clients get curious about their problems. By assisting clients in forming questions, we invite them to “climb up” with us, if you will, on an “observation deck” overlooking their lives where we may begin to look jointly for answers. Many clients report that they feel relief immediately after an initial assessment session simply from having translated their inner turmoil into concrete questions. Some clinicians would say the procedure helps engage the observing ego. I believe developmental affective neurobiologists like Schore (1994) and Siegel (1999) would tell us that we are actually helping people engage a different part of their brains, and that this helps them grow and develop.
Step 5—Written Feedback Is Provided
Clients’ assessment questions also gave an innovative way to structu...