
eBook - ePub
Health of HIV Infected People
Food, Nutrition and Lifestyle with Antiretroviral Drugs
Ronald Ross Watson, Ronald Ross Watson
This is a test
Compartir libro
- 632 páginas
- English
- ePUB (apto para móviles)
- Disponible en iOS y Android
eBook - ePub
Health of HIV Infected People
Food, Nutrition and Lifestyle with Antiretroviral Drugs
Ronald Ross Watson, Ronald Ross Watson
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Health of HIV Infected People: Food, Nutrition and Lifestyle with Antiretroviral Drugs provides basic and applied knowledge on the supportive roles of bioactive foods, exercise, and dietary supplements on HIV/AIDS patients receiving antiretroviral drugs.
Approaches include the application of traditional herbs and foods aiming to define both the risks and benefits of such practices. Readers will learn how to treat or ameliorate the effects of chronic retroviral disease using readily available, cheap foods, dietary supplements, and lifestyle changes with specific attention to the needs of patients receiving antiretroviral drugs.
This work provides the most current, concise, scientific appraisal of the efficacy (or lack thereof) of key foods, nutrients, dietary plants, and behavioral shifts in preventing and improving the quality of life of HIV infected infants and adults, while also giving the needed attention to these complex and important side effects.
- Covers the role of nutrients in the prevention and treatment of HIV-induced physiological changes in children undergoing HAART, including covers of omega-3 fatty acids, dietary fat intake, metabolic changes, and vitamin D
- Explores food and the treatment of obesity, diabetes, and cardiovascular disease in HIV infected patients, including fundamental coverage and recommendations for care
- Provides coverage of fitness and exercise regimens, physical activity, and behavioral and lifestyle changes on HIV infected individuals
- Gives careful attention to the specific nutritional needs of patients undergoing HAART therapy
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Health of HIV Infected People un PDF/ePUB en línea?
Sí, puedes acceder a Health of HIV Infected People de Ronald Ross Watson, Ronald Ross Watson en formato PDF o ePUB, así como a otros libros populares de Technology & Engineering y Food Science. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
Información
Categoría
Technology & EngineeringCategoría
Food ScienceSection III
Nutritional Issues in HIV/AIDs Patients: Focus on Antiretroviral Treated Populations
Outline
Chapter 15
Interactions Between Antiretrovirals and Natural Health Products
Christine Hughes1, Muhammed Zafar Iqbal Hydrie2 and Sunita Vohra3, 1Faculty of Pharmacy & Pharmaceutical Sciences, University of Alberta, Edmonton, AB, Canada, 2CARE Program for Integrative Health & Healing, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada, 3Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada
Patients with human immunodeficiency virus (HIV) frequently use natural health products in combination with antiretroviral therapy (ART). Several natural health products have been shown to interact with antiretroviral agents, which could result in therapeutic failure and development of HIV drug resistance. However, data on the interaction between natural health products and antiretroviral drugs are limited and are primarily based on small studies in subjects without HIV. Additional pharmacokinetic and clinical studies are needed in patients with HIV on newer antiretroviral regimens in combination with Western, African, or Traditional Chinese Herbal Medicines. In the meantime, health care providers need to be vigilant with regard to the possibility of interactions between natural health products and antiretroviral drugs in their patients.
Keywords
Antiretroviral; herbs; natural health products; HIV; adverse reactions; interactions
15.1 Background
The treatment of human immunodeficiency virus (HIV) infection has improved significantly after the introduction of combination antiretroviral therapy (cART), defined as use of a minimum of three active antiretroviral agents, which has resulted in reduced incidence of opportunistic infections and near-normal life expectancy [1,2]. Recent advances in ART include reduced pill burden due to increased availability of fixed-dose combination medications, as well as improved tolerability to newer antiretroviral drugs [1]. However, despite these advances, no cure has been found for HIV infection, and patients experience a multitude of physical symptoms as well as psychosocial issues, including stigma, isolation, and depression. Individuals with HIV also have higher rates of non-acquired immune deficiency syndrome (AIDS)–related disorders, including cardiovascular, kidney, and liver diseases; neurologic impairment; and certain cancers [3]. Due to the chronic nature of HIV infection and related conditions and their impact on quality of life, patients with HIV often seek complementary and alternative therapies.
On average, approximately 60% of patients with HIV report using complementary and alternative medicine (CAM), most commonly agents such as vitamins, herbs, and supplements [4–8]. Studies have shown that patients with HIV primarily use CAM as a complementary measure rather than as an alternative to antiretroviral therapy. The most common reasons for using CAM reported by patients with HIV are to increase energy level, to boost immunity, and to relieve side effects of antiretrovirals [4,6,8]. Patients have also reported using CAM to self-manage health or to gain a sense of control, attempt to normalize health status, or find wellness, as well as follow cultural values [9]. Demographic correlates of CAM use most commonly include Caucasian race compared with other races, male homosexuality compared with other sexual orientations, female gender, higher levels of education, and higher incomes [8–10]. HIV-related predictors of CAM use include longer duration of disease and ART, using a higher number of medications, and the presence of side effects of antiretrovirals [8,9]. Although most studies found that patients who used CAM did not reject conventional medicine [11–15], some studies have noted that CAM use is associated with nonadherence or the decision to not initiate ART [16,17].
Although there is a perception that natural health products (NHPs) are “natural” and therefore have low risks, the use of NHPs may be particularly problematic in patients with HIV due to the risk of NHP–drug interactions and overlapping toxicities, which can lead to treatment failure. One study found that of the 293 patients with HIV included in the study, 10% were advised to stop taking CAM due to concerns about serious drug interactions with ART or the adverse effects of CAM; 15% were advised to use CAM with caution due to potential interactions [5]. However, health care professionals do not yet routinely ask patients about use of NHPs, and studies have found that patient disclosure about CAM use varies considerably, between 38% and 90% [8]. This chapter provides an overview of the mechanisms of drug interactions between NHPs and antiretroviral drugs, pharmacokinetic and pharmacodynamic interactions, and recommendations for screening patients for potential interactions between antiretrovirals and NHPs. For the purposes of this chapter, NHPs include vitamin and minerals, herbal remedies, probiotics, traditional medicine, and homeopathic medicines, as well as other products such as amino acids and essential fatty acids [18].
15.2 Mechanisms of Drug Interactions with Antiretrovirals
Depending on the mechanism, drug interactions can be classified as either pharmacokinetic or pharmacodynamic. Pharmacokinetic interactions alter the absorption, distribution, metabolism, or excretion of another agent, whereas pharmacodynamic interactions lead to additive, synergistic, or antagonistic responses to drug therapy [19]. Antiretroviral drugs are frequently prone to pharmacokinetic drug–drug interactions as a result of the altered metabolism of the antiretroviral, the co-administered drug, or both or through the effects on transport proteins in the liver or intestine [19]. Drug interactions can result in an increased or decreased concentration of the antiretroviral drug, the co-administered agent, or both, resulting in either increased toxicity or therapeutic failure. Therapeutic failure of antiretroviral drugs is particularly worrisome, as it can lead to development of drug resistance, resulting in mutations and limiting future antiretroviral treatment options. There are more than 20 approved antiretroviral drugs that belong to six different medication classes [1] (Table 15.1). The non-nucleoside reverse transcriptase inhibitor (NNRTI) and protease inhibitor (PI) drug classes, chemokine receptor-5 antagonists (e.g., maraviroc), and integrase inhibitors (elvitegravir) are primarily metabolized by CYP3A4 in the liver. PIs are also substrates for P-glycoprotein and are inhibitors of CYP3A4, with ritonavir being the most potent [19]. Ritonavir is frequently used in low doses (100–200 mg/day) to “boost” the concentrations of co-administered PIs [1]. Ritonavir also inhibits CYP2D6 in the liver and induces CYP2C19, CYP2C9, and CYP1A2, increasing the risk for drug–drug interactions [19]. The NNRTIs efavirenz, nevirapine, and etravirine are inducers of CYP3A4; efavirenz and nevirapine are also inducers of CYP2B6 [19]. In addition, efavirenz and etravirine are inhibitors of CYP2C9 and CYP2C19. The integrase inhibitors, raltegravir and dolutegravir, have a lower potential for interactions, as these agents are primarily metabolized by uridine diphosphate glucuronosyltransferase (UGT) 1A1. Dolutegravir is also a substrate of CYP3A4 and P-glycoprotein in vitro [20]. Elvitegravir, however, is co-formulated with cobicistat, a potent inhibitor of CYP3A4, which is used to boost concentrations of elvitegravir but is also prone to interactions with other co-administered drugs [21]. Nucleoside reverse transcriptase inhibitors (NRTIs) are primarily renally cleared, and thus, pharmacokinetic interactions are less likely.
Table 15.1
Antiretroviral Agents
| NUCLEOSIDE/NUCLEOTIDE REVERSE TRANSCRIPTASE INHIBITORS | |
| Abacavir | Stavudine |
| Didanosine | Tenofovir |
| Emtricitabine | Zidovudine |
| Lamivudine | |
| NON-NUCLEOSIDE REVERSE TRANSCRIPTASE INHIBITORS | |
| Delavirdine | Nevirapine |
| Efavirenz | Rilpivirine |
| Etravirine | |
| PROTEASE INHIBITORS | |
| Atazanavir | Nelfinavir |
| Darunavir | Ritonavira |
| Fosamprenavir | Saquinavir |
| Indinavir | Tipranavir |
| Lopinavir | |
| INTEGRASE INHIBITORS | |
| Dolutegravir | Raltegravir |
| Elvitegravir | |
| CCR5 RECEPTOR ANTAGONISTS | |
| Maraviroc | |
| FUSION INHIBITORS | |
| Enfuvirtide | |
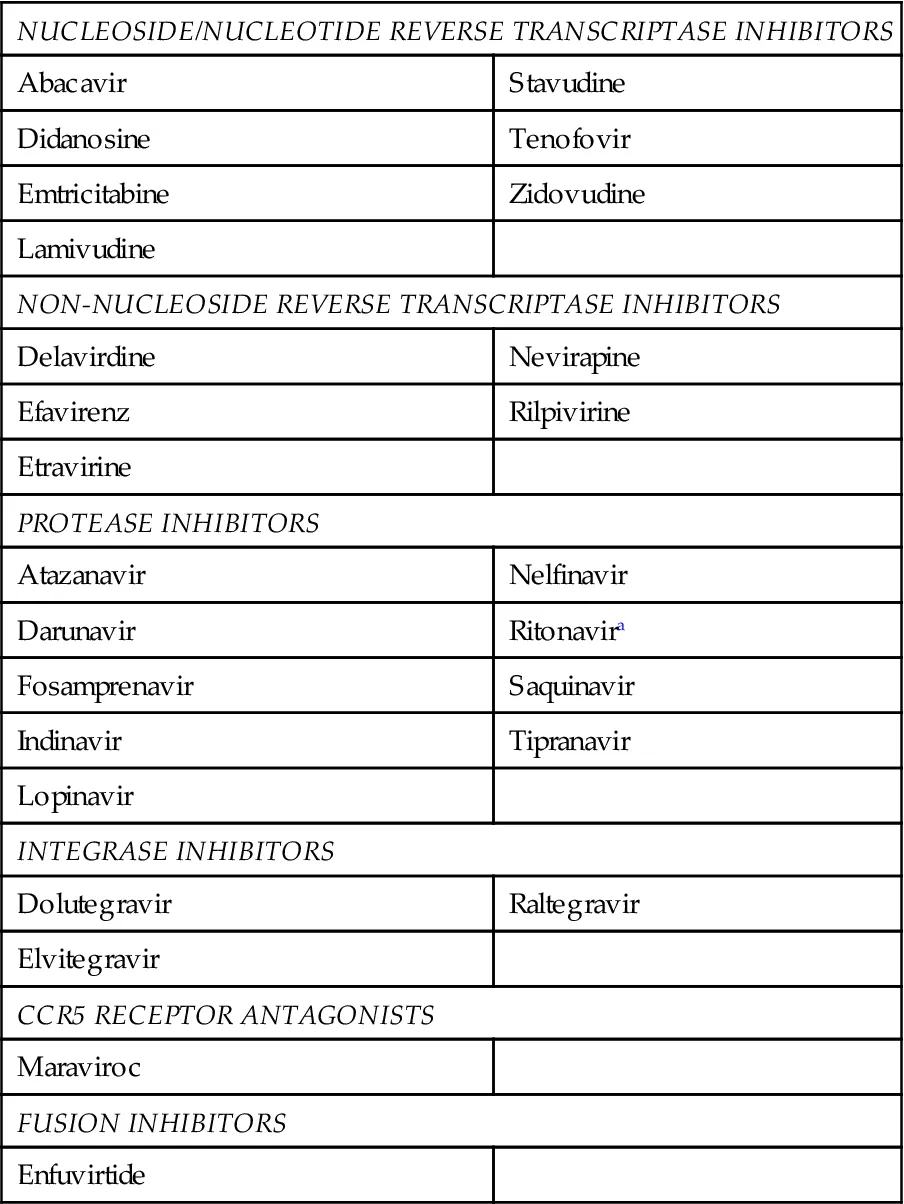
aLow-dose ritonavir and cobicistat are used as pharmacokinetic boosters for select antiretrovirals.
15.3 Pharmacokinetic Interactions Between Antiretrovirals and NHPs
Despite the prevalence of NHP use in patients with HIV, only a limited number of studies have been performed to assess NHP–antiretroviral drug interactions. A literature search of the Medline, Embase, CINAHL, and Cochrane Central Register of Controlled Trials (up to June 2014) databases has ...