Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors
Diagnosis and Management
Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr, Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr
This is a test
This is a test
Compartir libro
English
ePUB (apto para móviles)
Disponible en iOS y Android
eBook - ePub
Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors
Diagnosis and Management
Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr, Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr
Detalles del libro
Vista previa del libro
Índice
Citas
Información del libro
Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and Management is a modern, expertly crafted and clinically focused guide to the diagnosis, management and best-practice care of patients suffering from pancreatic cancer, cystic neoplasms and endocrine tumours.
Packed with outstanding figures and with reference to the leading society guidelines, its main focus is on the many endoscopic and radiologic diagnostic techniques, medical and surgical management of both full-blown cancer and other tumors, and the risks of each form of treatment. Also covered in detail are issues of tumor recurrence and long-term outcome of treatment.
Brought to you by highly skilled national and international leaders in the specialty and an experienced editor team, this is an invaluable guide to practicing gastroenterologists and surgeons in the hospital and clinical environment, as well as oncologists and endocrinologists managing patients with pancreatic tumorous lesions.
Preguntas frecuentes
¿Cómo cancelo mi suscripción?
Simplemente, dirígete a la sección ajustes de la cuenta y haz clic en «Cancelar suscripción». Así de sencillo. Después de cancelar tu suscripción, esta permanecerá activa el tiempo restante que hayas pagado. Obtén más información aquí.
¿Cómo descargo los libros?
Por el momento, todos nuestros libros ePub adaptables a dispositivos móviles se pueden descargar a través de la aplicación. La mayor parte de nuestros PDF también se puede descargar y ya estamos trabajando para que el resto también sea descargable. Obtén más información aquí.
¿En qué se diferencian los planes de precios?
Ambos planes te permiten acceder por completo a la biblioteca y a todas las funciones de Perlego. Las únicas diferencias son el precio y el período de suscripción: con el plan anual ahorrarás en torno a un 30 % en comparación con 12 meses de un plan mensual.
¿Qué es Perlego?
Somos un servicio de suscripción de libros de texto en línea que te permite acceder a toda una biblioteca en línea por menos de lo que cuesta un libro al mes. Con más de un millón de libros sobre más de 1000 categorías, ¡tenemos todo lo que necesitas! Obtén más información aquí.
¿Perlego ofrece la función de texto a voz?
Busca el símbolo de lectura en voz alta en tu próximo libro para ver si puedes escucharlo. La herramienta de lectura en voz alta lee el texto en voz alta por ti, resaltando el texto a medida que se lee. Puedes pausarla, acelerarla y ralentizarla. Obtén más información aquí.
¿Es Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors un PDF/ePUB en línea?
Sí, puedes acceder a Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors de Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr, Hans G. Beger, Akimasa Nakao, John P. Neoptolemos, Shu You Peng, Michael G. Sarr en formato PDF o ePUB, así como a otros libros populares de Medicine y Gastroenterology & Hepatology. Tenemos más de un millón de libros disponibles en nuestro catálogo para que explores.
CHAPTER 1 Histologic Classification and Tumor Staging of Pancreatic Cancer
Akio Yanagisawa and Eiichi Konishi
Kyoto Prefectural University of Medicine, Kyoto, Japan
Histologic Classification of Pancreatic Ductal Neoplasms
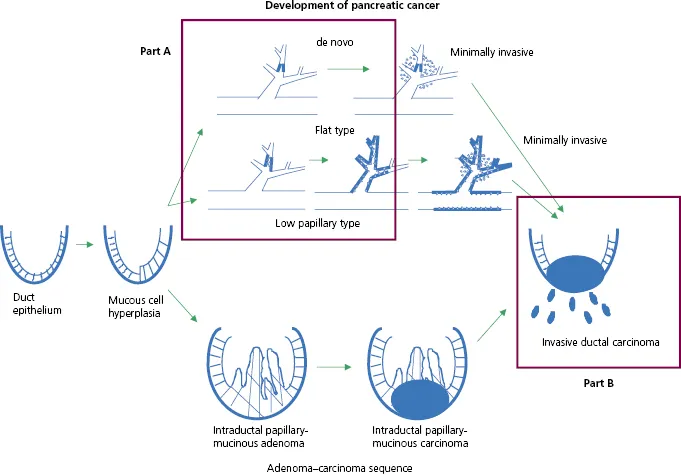
Ductal adenocarcinoma of the pancreas originates from the epithelium of the pancreatic duct and morphologically simulates it. To understand the classification of ductal adenocarcinomas of the pancreas correctly, it is important to know the basic rationale underlying the classification. Figure 1.1 shows the developmental pathway of the ductal adenocarcinoma, from ductal epithelium to invasive ductal carcinoma (1,2). The histological classification of the Japan Pancreas Society [Table 1.1 (Ref. 3)] and the World Health Organization (WHO) classification [Table 1.2 (Ref. 4)] have become widely accepted.
Figure 1.1 Developmental pathway of ductal adenocarcinoma, from ductal epithelium to invasive ductal carcinoma. Part A is classified as “carcinoma in situ” and Part B is classified as “invasive ductal carcinoma.”
Table 1.1 Histological classification and distribution of pancreatic ductal carcinoma in Japan, 2001–2007a
Number of patients
(%)
1 Atypical epithelium (AE) and carcinoma in situ (CIS)
14
(0.3)
2 Invasive ductal carcinomas (IDCs)
a Papillary adenocarcinoma (pap)
78
(1.4)
b Tubular adenocarcinoma (tub)
4564
(83.79)
i Well-differentiated type (tub1)
ii Moderately differentiated type (tub2)
c Poorly differentiated adenocarcinoma (por)
612
(11.2)
d Adenosquamous carcinoma (asc)
99
(1.8)
e Mucinous carcinoma (muc)
49
(1.0)
f Anaplastic carcinoma
37
(0.7)
i Giant cell type
ii Osteoclast-like giant cell type or giant cell carcinoma of osteoclastoid type
iii Pleomorphic type
iv Spindle-cell type
Total
5453
(100%)
a Data from Japanese Nationwide Pancreatic Cancer Registry. Courtesy of Japan Pancreas Society.
Table 1.2 WHO classification of tumors of the pancreatic ductal neoplasma
Undifferentiated carcinoma with osteoclast-like giant cells
a Data from Reference 4, Bosman et al., 2010.
According to the Japanese classification, Part A in Fig. 1.1 is classified as “carcinoma in situ” and Part B in Fig. 1.1 is classified as “invasive ductal carcinoma” and as “intraductal papillary mucinous neoplasm (IPMN), minimally invasive” or “IPMN, invasive.” Invasive ductal carcinoma is classified into six histological subtypes.
According to the WHO classification, Part A in Fig. 1.1 is classified as “pancreatic intraepithelial neoplasia (PanIN), grade 3” and Part B in Fig. 1.1 as “ductal adenocarcinoma” and “IPMN with an associated invasive carcinoma.” Ductal adenocarcinoma is also classified into six histological subtypes.
There is no significant difference between these two classification systems. This chapter discusses histological features of ductal adenocarcinoma according to the Japanese classification. IPMN is separately discussed in Section III, Chapters 27–39.
Atypical Epithelium and Carcinoma insitu
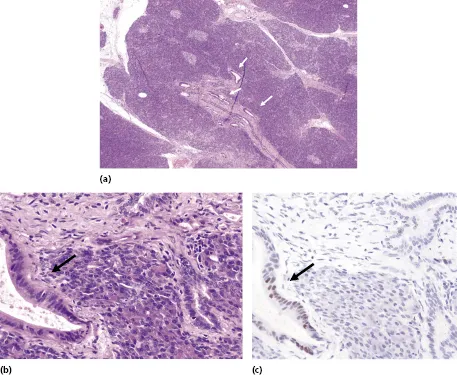
Carcinoma in situ (CIS) is a carcinoma limited to the pancreatic duct (Fig. 1.2 and Fig. 1.3a). Unlike IPMN, the duct affected with CIS is usually not dilated markedly and the dilatation is usually less than 5 mm. Histologically, it shows a completely flat or low papillary growth of atypical cells. The diagnosis of malignancy is usually based on cytologic atypia. On immunohistochemistry, p53 may be diffusely or strongly positive in the nuclei. This might be helpful in the differential diagnosis. Atypical epithelium (AE) is a lesion without as much cellular atypia as CIS.
Figure 1.2(a) Very small ductal adenocarcinoma (arrowheads), 3 mm in diameter. (b) Noninvasive ductal adenocarcinoma (left, arrow) and normal pancreatic duct (right). (c) Immunofluorescence shows the atypical duct (left, arrow) is positive for p53, but the normal pancreatic duct (right) is negative.
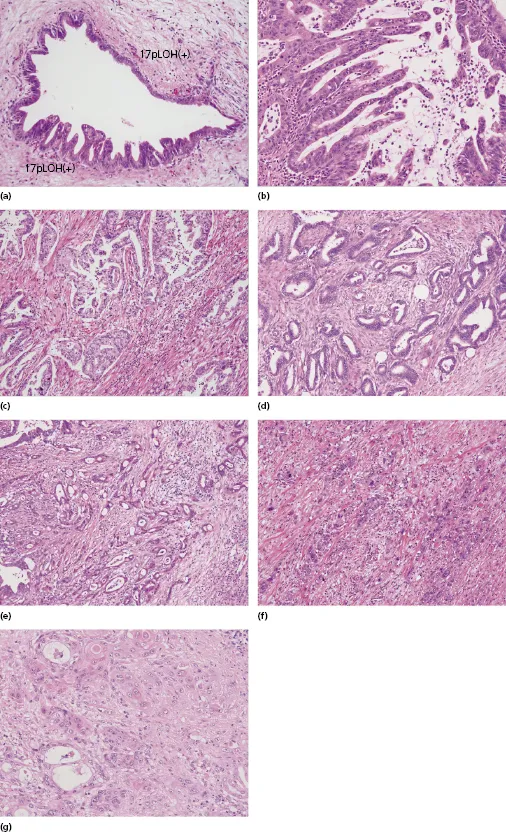
Figure 1.3 Differential variants of ductal adenocarcinoma: (a) carcinoma in situ, flat type and low papillary type; (b) papillary adenocarcinoma (pap); (c) papillotubular adenocarcinoma, well-differentiated type; (d) tubular adenocarcinoma, well-differentiated type (tub1); (e) tubular adenocarcinoma, moderately differentiated type (tub2); (f) poorly differentiated adenocarcinoma (por); (g) adenosquamous carcinoma (asc).
Invasive Ductal Carcinomas
Invasive ductal carcinomas (IDCs) are the most common neoplasm in the pancreas. According to the cancer registry of the Japan Pancreas Society (2001–2007), IDCs represent 74% of all pancreatic tumors (5449 of 7356 cases) and 82% of all pancreatic exocrine carcinomas (5449 of 6621 cases). The cut surface of an IDC is usually firm and fibrous. Medullary lesions, such as undifferentiated (anaplastic) carcinoma, are rarely present. Histologically, IDCs are subclassified into six subtypes. Tubular adenocarcinoma is the most common subtype (84% of IDCs; Table 1.1).
Papillary adenocarcinoma is an IDC with significant papillary growth pattern (0.3% of IDCs; Fig. 1.3b). This category should not include mucinous cystadenocarcinoma or adenocarcinoma arising from IPMN, with significant papillary pattern. These should be categorized as “invasive” mucinous cystadenocarcinoma or “invasive” IPMN. Tubular adenocarcinoma has two subtypes, well-differentiated type and moderately differentiated type, graded by the degree of glandular formation (Fig. 1.3c–e).
Poorly differentiated adenocarcinoma is classified separately from tubular adenocarcinoma in the Japanese classification (Fig. 1.3f). In the WHO classification (Table 1.2), however, it is classified as tubular adenocarcinoma.
Histopathological grade of differentiation, evaluated by tubular formation, has been reported as an insignificant factor for outcome. However, according to our analysis of the outcomes of the cases with radical pancreatectomy for tubular adenocarcinoma (21 cases, 2–6 cm in the greatest dimension) in Japan, the 5-year survival rate for the patients with well-differentiated tubular adenocarcinoma (27%, 5 of 15 cases) was better than that for the patients with moderately or poorly differentiated tubular adenocarcinoma (0%, 0 of 6 cases; p = 0.105). It is necessary to elucidate whether the histopathological grading affects the patient's prognosis or not.
It is not uncommon to see squamous differentiation in pancreatic carcinoma, but adenosquamous carcinoma represents 1.8% of all IDCs (99 of 5449 cases; Fig. 1.3g). Generally, it should have an area of squamous differentiation more than 25%–30% of the tumor; otherwise it should be classified as adenocarcinoma. Pure squamous cell carcinoma is extremely rare, because one can usually find an adenocarcinoma component when the tumor is examined thoroughly. Therefore, “squamous cell carcinoma” is not included in the classification. Even if one cannot find an area of adenocarcinoma by routine examination, the tumor should be d...