![]()
Part 1: Introduction to diabetes
Chapter 1
Introduction to diabetes
Diabetes mellitus is a condition of chronically elevated blood glucose concentrations which give rise to its main symptom of passing large quantities of sweet-tasting urine (diabetes from the Greek word meaning ‘a siphon’, as the body acts as a conduit for the excess fluid, and mellitus from the Greek and Latin for honey). The fundamental underlying abnormality is a net (relative or absent) deficiency of the hormone insulin. Insulin is essentially the only hormone that can lower blood glucose.
There are two categories of diabetes: type 1 is caused by an autoimmune destruction of the insulin-producing β cell of the islets of Langerhans in the pancreas (absolute deficiency); and type 2 is a result of both impaired insulin secretion and resistance to its action – often secondary to obesity (relative deficiency).
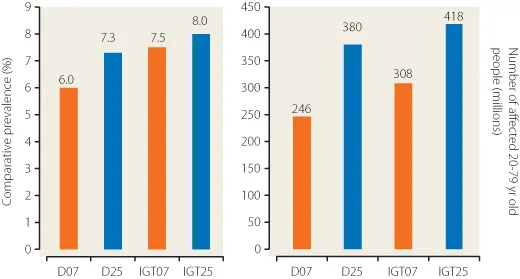
The precise level of blood glucose that defines diabetes has been revised several times and is covered in more detail in Chapter 3. Diabetes is common and is becoming more common. Age-adjusted prevalence is set to rise from 5.9% to 7.1% (246–380 million) worldwide in the 20–79 year age group, a 55% increase (Figure 1.1). The relative proportions of type 1 to type 2 vary from 15 : 85 for Western populations to 5 : 95 in developing countries.
It is the short- and long-term complications of diabetes which make it a major public health problem. Absolute deficiency of insulin leads to ketoacidosis and coma with an appreciable mortality even in the UK and other Western countries. Hyperglycaemic hyperosmolar coma (now called hyperglycaemic hyperosmolar state) is less common and more insidious but remains an equally serious problem for people with type 2 diabetes (see Chapter 12).
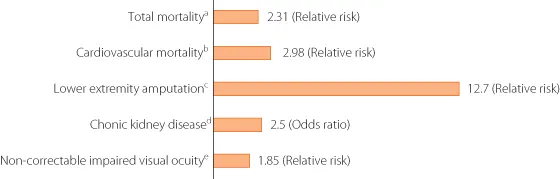
Long-term hyperglycaemia affects the microvasculature of the eye, kidney and nerve as well as the larger arteries, leading to accelerated atherosclerosis. Diabetes is the most common cause of blindness in those of working age, the most common single cause of end-stage renal failure worldwide, and the consequences of neuropathy make it the most common cause of non-traumatic lower limb amputation. Mortality from ischaemic heart disease and stroke is 2–4-fold higher than in the age- and sex-matched non-diabetic population. All these important clinical problems will be covered in detail in subsequent chapters (Figure 1.2).
This handbook sets out to cover the essentials of diagnosis, epidemiology and management of diabetes and its distressingly many complications. By using case vignettes and summaries of key trials together with web links and suggestions for further reading, it will serve as a useful desktop reference for all healthcare professionals who provide diabetes care.
FURTHER READING
International Diabetes Federation. Diabetes Atlas, 4th edn. Brussels: International Diabetes Federation, 2009.
KEY WEBSITE
- Diabetes Atlas: www.eatlas.idf.org
KEY POINTS
- Diabetes is common and its incidence is rising.
- Type 2 diabetes is by far the most common accounting for 85–95% of cases.
- Complications in the microvasculature (eye, kidney and nerve) and the macrovasculature are responsible for considerable morbidity and excess mortality.
![]()
Chapter 2
History of diabetes
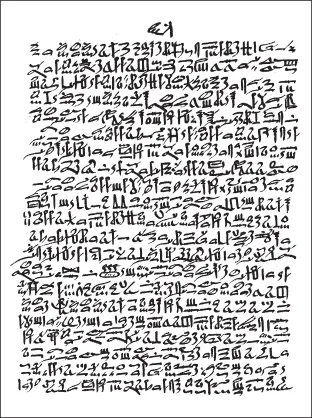
Diseases with the clinical features of diabetes have been recognised since antiquity. The Ebers papyrus (Figure 2.1), dating from 1550 BC, describes a polyuric state that resembles diabetes.
The word ‘diabetes’ was first used by Aretaeus of Cappadocia in the second century AD. Aretaeus gave a clinical description of the disease (Box 2.1), noting the increased urine flow, thirst and weight loss, features that are instantly recognizable today.
Box 2.1 Description of diabetes by Aretaeus
Diabetes is a dreadful affliction, not very frequent among men, being a melting down of the flesh and limbs into urine. The patients never stop making water and the flow is incessant, like the opening of aqueducts. Life is short, unpleasant and painful, thirst unquenchable, drinking excessive, and disproportionate to the large quantity of urine, for yet more urine is passed. One cannot stop them either from drinking or making water. If for a while they abstain from drinking, their mouths become parched and their bodies dry; the viscera seem scorched up, the patients are affected by nausea, restlessness and a burning thirst, and within a short time, they expire.
Adapted from Papaspyros S. The History of Diabetes Mellitus, 2nd edn. Stuttgart: Thieme, 1964.
The sweet, honey-like taste of urine in polyuric states, which attracted ants and other insects, was reported by Hindu physicians such as Sushrut (Susruta) during the fifth and sixth centuries AD. These descriptions even mention two forms of diabetes, the more common occurring in older, overweight and indolent people, and the other in lean people who did not survive for long. This empirical subdivision predicted the modern classification into type 1 and type 2 diabetes.
Diabetes was largely neglected in Europe until a 17th-century English physician, Thomas Willis (1621–75) (Figure 2.2), rediscovered the sweetness of diabetic urine. Willis, who was physician to King Charles II, thought that the disease had been rare in ancient times, but that its frequency was increasing in his age ‘given to good fellowship’. Nearly a century later, the Liverpool physician Matthew Dobson (1735–84) showed that the sweetness of urine and serum was caused by sugar. John Rollo (d. 1809) was the first to apply the adjective ‘mellitus’ to the disease.
In the 19th century, the French physiologist Claude Bernard (1813–78) (Figure 2.3) made many discoveries relating to diabetes. Among these was the finding that the sugar that appears in the urine was stored in the liver as glycogen. Bernard also demonstrated links between the central nervous system and diabetes when he observed temporary hyperglycaemia (piqûre diabetes) when the medulla of conscious rabbits was transfixed with a needle.
In 1889, Oskar Minkowski (1858–1931) and Joseph von Mering (1849–1908) from Strasbourg removed the pancreas from a dog to see if the organ was essential for life. The animal displayed typical signs of diabetes, with thirst, polyuria and wasting, which were associated with glycosuria and hyperglycaemia. This experiment showed that a pancreatic disorder causes diabetes, but they did not follow up on the observation.
Paul Langerhans (1847–88) (Figure 2.4) from Berlin, in his doctoral thesis of 1869, was the first to describe small clusters of cells in teased preparations of the pancreas. He did not speculate on the function of the cells, and it was Edouard Laguesse in France who later (1893) named the cells ‘islets of Langerhans’ and suggested that they were endocrine tissue of the pancreas that produced a glucose-lowering hormone.
In the early 20th century, several workers isolated impure hypoglycaemic extracts from the pancreas, including the Berlin physician Georg Zuelzer (1840–1949), the Romanian Nicolas Paulesco (1869–1931), and the Americans Ernest Scott (1877–1966) and Israel Kleiner (1885–1966).
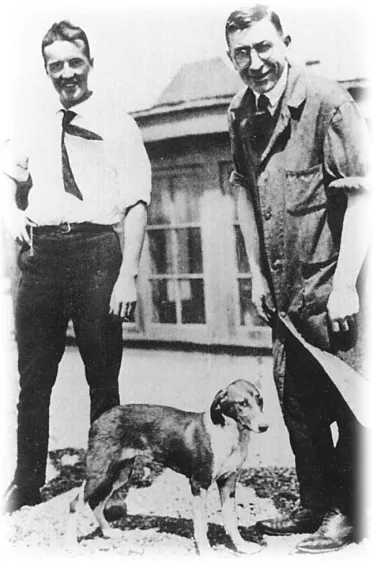
Insulin was discovered in 1921 at the University of Toronto, Canada, through a collaboration between the surgeon Frederick G Banting (1891–1941), his student assistant Charles H Best (1899–1978), the biochemist James B Collip (1892–1965) and the physiologist JJR Macleod (1876–1935). Banting and Best made chilled extracts of dog pancreas, injected them into pancreatectomised diabetic dogs, and showed a fall in blood gluocse concentrations (Figure 2.5).
Banting and Best’s notes of the dog experiments refer to the a...