Philip I. Aaronson, Jeremy P. T. Ward, Michelle J. Connolly
This is a test
This is a test
Partager le livre
English
ePUB (adapté aux mobiles)
Disponible sur iOS et Android
eBook - ePub
The Cardiovascular System at a Glance
Philip I. Aaronson, Jeremy P. T. Ward, Michelle J. Connolly
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
Everything you need to know about the cardiovascular system... at a Glance!
The Cardiovascular System at a Glance is the essential reference guide to understanding all things circulatory. Concise, accessible, and highly illustrated, this latest edition presents an integrated overview of the subject, from the basics through to application. Featuring brand new content on stroke, examination and imaging, heart block and ECGs, and myopathies and channelopathies, The Cardiovascular System at a Glance goes one step further and offers new and updated clinical case studies and multiple-choice questions on a supplementary website.
Integrates basic science and clinical topics
Offers bite-size chapters that make topics easy to digest
Includes coverage of anatomy and histology, blood and haemostasis, cellular physiology, form and function, regulation and integration of cardiovascular function, history, examination and investigations, pathology and therapeutics
Filled with highly visual, colour illustrations that enhance the text and help reinforce learning
The fifth edition of The Cardiovascular System at a Glance is an ideal resource for medical students, junior doctors, students of other health professions, and specialist cardiology nurses.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que The Cardiovascular System at a Glance est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à The Cardiovascular System at a Glance par Philip I. Aaronson, Jeremy P. T. Ward, Michelle J. Connolly en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medizin et Klinische Medizin. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
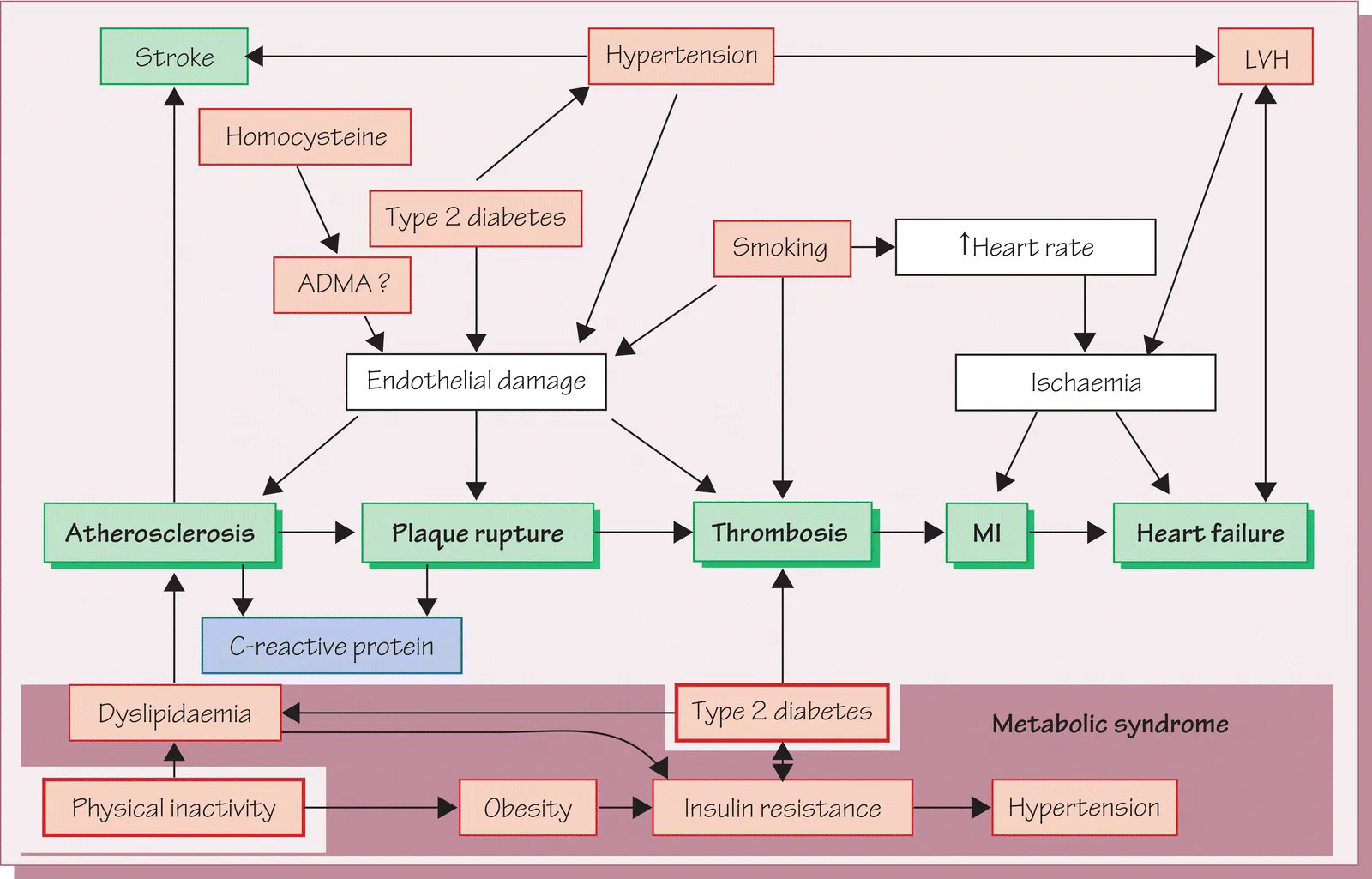
Figure 34.1 Relationships between risk factors and cardiovascular disease
The main manifestations of cardiovascular disease (CVD) are coronary heart disease (CHD), cerebrovascular disease (stroke) and peripheral vascular disease, and the underlying cause of these is most often atherosclerosis (see Chapter 37). Numerous factors or conditions are known to increase (or decrease) the probability that atherosclerosis will develop, and the presence in an individual of these cardiovascular risk factors can be used to assess the likelihood that overt cardiovascular morbidity and death will occur in the medium term (Figure 34.1).
Some risk factors such as age, male sex and family history of CVD are fixed. However, others, including dyslipidaemias, smoking, hypertension, diabetes mellitus, obesity and physical inactivity, are modifiable. These probably account for over 90% of the risk of developing atherosclerotic CVD. The attempt to prevent CVD by targeting modifiable risk factors has become a cornerstone of modern disease management because the occurrence of overt CVD is preceded by the development of subclinical atherosclerosis which takes many years to progress.
Figure 34.1 illustrates the main mechanisms by which major risk factors are thought to promote the development of atherosclerosis and its most important consequence, CHD. Additional aspects of dyslipidaemias and hypertension are described in Chapters 36–39.
Modifiable risk factors
Dyslipidaemias are a heterogeneous group of conditions characterized by abnormal levels of one or more lipoproteins. Lipoproteins are blood‐borne particles that contain cholesterol and other lipids. They function to transfer lipids between the intestines, liver and other organs (see Chapter 36).
Dyslipidaemias involving excessive plasma concentrations of low‐density lipoprotein (LDL) are associated with rises in plasma cholesterol levels, because LDL contains 70% of total plasma cholesterol. As the level of plasma cholesterol rises there is a progressive increase in the risk of CVD due to the attendant rise in LDL levels. LDL has a pivotal role in causing atherosclerosis because it can be converted to an oxidized form, which damages the vascular wall (see Chapter 37). Drugs that lower plasma LDL (and therefore oxidized LDL) slow the progression of atherosclerosis and reduce the occurrence of CVD. Elevated levels of lipoprotein (a), a form of LDL containing the unique protein apo(a), have been reported to confer additional cardiovascular risk. Apo(a) contains a structural component closely resembling plasminogen, and it may inhibit fibrinolysis (see Chapters 8 and 45) by competing with plasminogen for endogenous activators. High levels of plasma triglycerides may also be correlated with CVD, although this remains controversial.
On the other hand, the risk of CVD is inversely related to the plasma concentration of high‐density lipoprotein (HDL), possibly because HDL functions to remove cholesterol from body tissues, and may act to inhibit lipoprotein oxidation. The LDL+HDL (total cholesterol): HDL cholesterol ratio is therefore a better predictor of risk than the LDL level. Hypertension occurs in almost 30% of the population and in more than half of people who are middle aged or older. Hypertension promotes atherogenesis, probably by damaging the endothelium and causing other deleterious effects on the walls of large arteries. Hypertension damages blood vessels of the brain and kidneys, increasing the risk of stroke and renal failure. The higher cardiac workload imposed by the increased arterial pressure also causes a thickening of the left ventricular wall. This process, termed left ventricular hypertrophy (LVH), is both a cause and harbinger of more serious cardiovascular damage. LVH predisposes the myocardium to arrhythmias and ischaemia and is a major contributor to heart failure, myocardial infarction (MI) and sudden death.
Physical inactivity promotes CVD via multiple mechanisms. Low fitness is associated with reduced plasma HDL, higher levels of blood pressure and insulin resistance, and obesity, itself a CVD risk factor. Studies show that a moderate to high level of fitness is associated with a halving of CVD mortality.
Diabetes mellitus is a metabolic disease present in approximately 5% of the population. Diabetics either lack the hormone insulin entirely or become resistant to its actions. The latter condition, which usually develops in adulthood, is termed type 2 diabetes mellitus (DM2), and accounts for 95% of diabetics. Diabetes causes progressive damage to both the microvasculature and larger arteries over many years. Approximately 75% of diabetics eventually die from CVD.
There is evidence that patients with DM2 have both endothelial damage and increased levels of oxidized LDL. Both effects may be a result of mechanisms associated with the hyperglycaemia characteristic of this condition. Also, blood coagulability is increased in DM2 because of elevated plasminogen activator inhibitor 1 (PAI‐1) and increased platelet aggregability.
A set of cardiovascular risk factors including high plasma triglycerides, low plas...