The full-arch implant rehabilitation (FAIR) protocol is one of the newest implant therapy innovations to treat the edentulous or nearly edentulous patient. The FAIR prosthesis is immediate, fixed, esthetically pleasing, highly functional, inexpensive, and maintainable, and it can frequently be installed without bone grafting. This book describes how the FAIR protocol works, who it should be used for, and methods to implement it successfully for different patients. The system can be used in both arches and in patients with total or near-total edentulism. Several chapters are devoted to describing step-by-step treatment with detailed clinical photographs documenting every step from initial assessment to prosthesis delivery. Even those new to fixed denture systems will find the procedures easy to follow and can begin implementing the FAIR approach for their patients.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Full-Arch Implant Rehabilitation est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Full-Arch Implant Rehabilitation par Arun Garg en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Dentistry. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
The full-arch implant rehabilitation (FAIR) protocol is one of the newest innovations in implant therapy to treat the edentulous or nearly edentu-lous patient. Instead of single implants replacing individual missing teeth, four or five implants are spaced throughout the arch and immediately loaded with a provisional fixed prosthesis. While conventional removable dentures and bone grafting with multiple implants are other options, the latter can take several years and has commensurate high costs. Morever, a number of studies have shown that wearing conventional removable dentures can reduce patients’ quality of life, causing pain and areas of discomfort, chewing and speaking difficulties, slippage, reduced occlusal force, and poor oral sensation.
The FAIR dental prosthesis offers many advantages for the dental patient with a fully or partially edentulous arch (Table 1-1). The prosthesis is immediate, fixed, esthetically pleasing, highly functional, inexpensive, and maintainable. Importantly, the FAIR procedure and similar techniques can frequently be performed without bone grafting with exceptional success rates.1–14 Such dental systems are better designed to meet the surgical and restorative needs of more patients with edentulous or partially edentulous arches, because traditional techniques often require extensive bone grafting. The invasiveness of these procedures deters many patients, and others (particularly elderly patients and those with severe bone loss) may not be good candidates for bone grafting.
TABLE 1-1 Advantages and disadvantages of removable dentures, overdentures, and the FAIR approach
ADVANTAGES
DISADVANTAGES
Removable dentures
▪ Relatively inexpensive tooth and gingival replacement
▪ Provides lip support
▪ Easy to remove and clean outside of the mouth
▪ Uncomfortable
▪ May cause sore spots on gingival tissue
▪ Makes it difficult to eat certain foods
▪ Causes accelerated bone loss
▪ Often requires relining to improve comfort as bone deteriorates
▪ May make speech difficult
▪ May require creams or adhesives to reduce mobility
▪ Approximately 10% functionality compared with natural teeth
Removable overdenture supported by 2 or 4 implants
▪ Improves stability and functionality to 60% compared with natural teeth
▪ Relatively inexpensive tooth and gingival replacement
▪ Provides lip support
▪ Easy to clean outside of the mouth
▪Uncomfortable
▪ May cause sore spots on gingival tissue
▪ Denture must be removed and cleaned outside of the mouth
▪ May still move when chewing or speaking
▪ May require relining to improve fit and comfort as bone deteriorates
FAIR approach
▪ Improves functionality to 70% compared with natural teeth
▪ Eliminates the need for bone grafting
▪ A provisional partial denture can be provided on the day of surgery, allowing a soft food diet during healing
▪ Replaces roots and teeth
▪ Preserves bone and soft tissue
▪ No decay; 95% success rate over 30 years
▪ Natural-looking esthetics
▪ Allows patients to eat any kinds of foods
▪ Can be cleaned like natural teeth
▪ Requires healing and restorative time
▪ Involves surgical procedure and anesthesia
During the late 1980s and early 1990s, the success rates for immediately loaded implants improved, both for the restoration of individual teeth and the placement of short-span fixed partial dentures.15–20 These developments served to push the envelope toward full-arch replacement, both with and eventually without bone grafting. The mid to late 1990s saw the development of mandibular restoration protocols that attempted to meet the challenges of anatomical placement and a redesigned partial denture architecture in the dense bone of the mandible.21,22 Similar attempts in the softer, more porous maxillary bone were generally unsuccessful because of poor anchorage.23–28 To overcome this challenge, the threading, size, and length of implants were redesigned to condense and thicken bone during placement in soft bone and with sinus elevation and other procedures.29–32
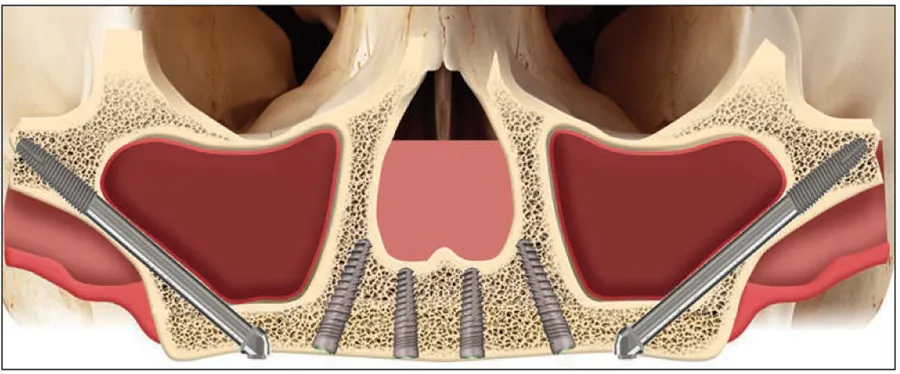
The early 2000s saw significant improvement in the esthetics of fixed prosthodontics, particularly with the introduction of pink ceramic for the gingiva. Retrospective studies of fixed full-arch prostheses in the mandible and zygomatic implants in the maxilla showed how protocols for full-arch dental prostheses had evolved.33–37 For example, when traditional implant surgery and bone grafting for sinus elevation and other procedures are contraindicated in the maxilla due to patient age or other issues with bone density or availability, the longer, nontraditional zygomatic implants can be placed near the dense, more cortical cheek bone (ie, zygoma) in the posterior maxilla (Fig 1-1). This decreases the time needed for the procedure and increases patient comfort.38,39 By about 2010, additional advancements in implant design and protocols included techniques for extramaxillary anchorage, optimal implant angulation, optional use of cantilevers, and bone reduction (when required).40–45
Fig 1-1 Placing zygomatic implants near the dense, more cortical cheekbone in the posterior maxilla is an example of an early evolution in protocol for full-arch dental prostheses.
An earlier treatment option for edentulous patients that reflects the evolution of dental implant technology is the two- or four-implant removable overdenture.46–48 Unlike conventional removable dentures (Fig 1-2), the fixed removable overdenture improves stability and function to approximately 60% that of natural teeth (Fig 1-3) and yet is still relatively inexpensive as a replacement for teeth and gingiva. Additionally, it provides lip support and easy cleaning outside the mouth. Disadvantages include sore spots on the gingiva, some movement when the patient chews and speaks, and the possible need for frequent relining for fit and comfort because of continued bone resorption.
Fig 1-2 The conventional denture was a first step in the evolution toward the FAIR protocol.
Fig 1-3 The fixed removable overdenture improves stability and function to approximately 60% that of natural teeth.
The FAIR Difference
In contrast, the FAIR prosthesis and other similar protocols have only two requirements that could be considered disadvantages: a surgical procedure and a short period afterward for healing and restoration. For these relatively minor disadvantages, the FAIR protocol (Fig 1-4) provides 70% of the functionality of natural teeth, requires minimal or no grafting before placement, and serves as a replacement for bone and teeth (preserving both bone and soft tissue). A provisional prosthesis is delivered on the day of surgery, allowing the consumption of soft foods during healing. The definitive ...