
eBook - ePub
Essentials of Orthognathic Surgery
Second Edition
Johan P. Reyneke
This is a test
Partager le livre
- 280 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Essentials of Orthognathic Surgery
Second Edition
Johan P. Reyneke
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
The revised edition of this essential text presents a concise approach to the diagnosis and surgical treatment of dentofacial deformities encountered in clinical practice. The treatment process and the most common surgical techniques are featured in step-by-step protocols. The contents have been updated to reflect the most current interpretation of diagnostic data, including expanded discussions of the rotation of the maxillomandibular complex and anterior open bite dentofacial deformities as well as new sections on distraction osteogenesis and the intraoral vertical mandibular ramus osteotomy.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Essentials of Orthognathic Surgery est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Essentials of Orthognathic Surgery par Johan P. Reyneke en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicina et Odontotecnica. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
chapter 1
Principles of Orthognathic Surgery
Peopl eusually recognize malpositioned teeth or obvious jaw deformities and seek treatment from an orthodontist, who can improve tooth alignment, function, and facial esthetics. More severe deformities that require a combination of orthodontics and surgery for correction are called dentofacial deformities. These deformities can affect physical orofacial function in several ways. Mastication can be impaired, and, especially in severe cases, this impairment can affect digestion and general nutritional health. Lip incompetence due to excessive vertical growth of the maxilla results in mouth breathing, which eliminates the physiologic effect of the nose on breathing. Speech is often affected by dentofacial deformities despite adaptive capabilities of the body. Malpositioned teeth may have a profound effect on maintenance of proper oral hygiene, thus making teeth more susceptible to dental caries and periodontal disease. Normal temporomandibular function is also often affected by several types of dentofacial deformities.
The physical effects of a dentofacial deformity are important, but the psychosocial impact of a dentofacial deformity on an individual is often paramount. Such a deformity can profoundly affect the quality of life and entail lifelong adjustment.
The combination of surgery and orthodontic treatment makes it possible to treat dentofacial deformities that previously could not have been corrected orthodontically (eg, vertical maxillary excess and severe anterior open bite malocclusion). Orthognathic surgery has created new and exciting opportunities in the treatment of patients with dentofacial deformities and provided the orthodontist with options other than compromised treatment for patients with skeletal disharmony. Experience in orthognathic surgery, an increased understanding of its biologic basis, and a refinement of its art form now enable us to routinely deliver a stable, esthetic, and functional result to patients.
Three kinds of treatment are available when malocclusion is caused by severe skeletal discrepancies:
- Growth modification. In growing children, dentofacial orthopedics can alter the expression of growth to some extent. (How much growth can be altered varies, and this topic remains controversial.) Facial growth patterns that may be influenced by growth modification in the adolescent include the following:
- Maxillary anteroposterior excess: Excessive horizontal growth of the maxilla may be retarded by headgear or camouflaged by extraction of upper first bicuspids and orthodontic retraction of the incisors.
- Maxillary anteroposterior deficiency: Moderate improvement can be established by orthodontic protraction.
- Vertical maxillary excess: High-pull headgear of temporary anchorage devices can retard the vertical growth of the maxilla and diminish the severity of the deformity.
- Mandibular anteroposterior deficiency: Headgear combined with functional appliances have the potential to improve mandibular projection. Skeletal deformities such as mandibular anteroposterior excess, vertical maxillary deficiency, and microgenia cannot be easily influenced by growth modification.
- Orthodontic camouflage. There is a group of patients with mild skeletal discrepancy that would benefit from orthodontic camouflage and not surgery. Dental compensation for a skeletal deformity, or orthodontic camouflage, may be associated with impaired esthetics, questionable posttreatment stability, and prolonged treatment time.
- Orthognathic surgery. Combined orthodontic and surgical correction is considered the best treatment modality for dentoskeletal imbalances once growth has ceased. Although orthognathic surgery is associated with certain risks and challenges, it has become a more refined and less traumatic procedure for patients and therefore has become a reasonable treatment option. The remarkable facial changes created by improved skeletal relationships have become an important factor in treatment goal-setting.
Patients seeking orthodontic treatment have a wide range of functional and esthetic needs and can be divided into three groups:
Group 1: Those with normal skeletal relationship and malocclusions that can be treated using routine orthodontic techniques.
Group 2: Those with mild to moderate skeletal discrepancies. The malocclusions of many of the patients in this group can be corrected by dental compensation and growth management.
Group 3: Those with moderate to severe skeletal discrepancy and noticeable facial imbalance. The negative effects of compromised orthodontic treatment for patients in the third group would be unacceptable, making combined surgery and orthodontics the treatment of choice.
An important challenge for the clinician is to differentiate between borderline group 2 and group 3 patients. Treatment of patients who belong in group 3 with orthodontic camouflage would be a mistake, just as surgical treatment of certain patients who belong in group 2 would be inappropriate. The decision regarding the best treatment for borderline group 2 and group 3 patients is influenced by various factors:
- The patient’s main complaint and preferences. Some patients are interested only in improving occlusion whereas esthetic change is a high priority for others.
- The orthodontist’s preferences and skills. The orthodontist’s confidence in surgical outcomes may have been influenced by previous poor surgical results; there will be a natural hesitation to continue to recommend surgery to patients based on past experience.
- Available surgical skills. Orthognathic surgical expertise may not be available in the area, and the patient may be unable to travel.
- Lack of insurance coverage. The financial implications of orthodontic treatment with the added burden of surgery and hospitalization can be substantial and is a significant factor for patients to consider.
Treating patients in group 3 with orthodontics alone (group 2 treatment) may create additional problems, such as occlusal relapse, worsening of the profile, and periodontal and temporomandibular joint decline, rather than solve the existing problem. Surgical treatment of patients in group 2 is appropriate when camouflage treatment would produce an unacceptable esthetic result or when orthodontics alone cannot achieve the desired facial change. Camouflage treatment also can be defined as an alternative treatment method that should render acceptable functional, stable, and esthetic results.
Treatment Objectives in Orthognathic Surgery
Three treatment objectives are fundamental in orthognathic surgery: (1) function, (2) esthetics, and (3) stability. These three objectives form the basis of goals in treating patients with dentofacial deformities and often go hand in hand.
Function
Functional and esthetic deformities often exist concurrently; when they do, treatment should be designed to correct both. When correcting a functional problem, the clinician should make full use of the opportunity to improve facial esthetics at the same time. The treatment of patients with poor function but good esthetics is particularly challenging. Careful planning is essential to avoid additional esthetic deformity while providing optimal functional relationships.
Esthetics
Facial appearance is often the patient’s main concern. It is the patient’s perception of what is esthetically wrong that is paramount, and one of the clinician’s first tasks is to establish the patient’s esthetic concerns. As Leo Tolstoy said in Childhood, “I am convinced that nothing has so marked influence on the direction of a man’s mind as his appearance, and not his appearance itself so much as his conviction that it is attractive or unattractive.”
Esthetic imbalance is often the result of a significant dentoskeletal deformity. In some patients esthetic results can be improved by surgery alone, although the functional problem will not necessarily be treated. An example is accepting a Class II malocclusion after surgical advancement of the chin for a patient with mandibular anteroposterior deficiency. In contrast, for a patient with vertical maxillary excess it may be possible to achieve a Class I malocclusion by orthodontic treatment alone; however, an ideal esthetic result is not possible.

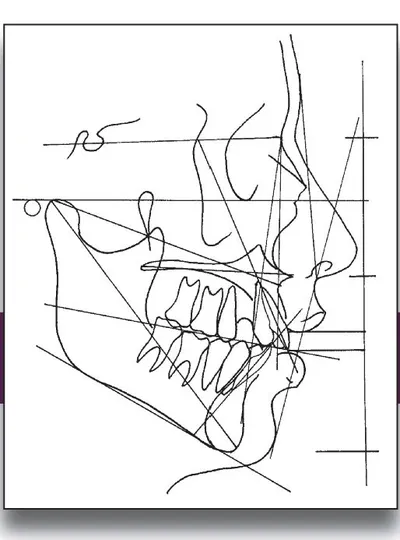
Figs 1-1a to 1-1e This 20-year-old patient was referred to the surgeon with the main complaint that her chin appeared too small and she did not like her “gummy smile.” Previous orthodontic treatment lasted 3 years and consisted of extraction of four first premolars, retraction of maxillary incisors, and proclination of mandibular incisors. She was not offered the option of surgical correction of her skeletal problem. (a) Frontal view. (b) Profile. (c) Smile. The dental compromise for the skeletal disharmony is evident in the occlusion (d) and the cephalometric analysis (e). The ideal treatment for this patient would have been the preoperative orthodontic creation of a Class II malocclusion (possibly with a different extraction pattern), followed by the vertical repositioning of her maxilla and advancement of her mandible.
Because the orthodontic placement of the teeth dictates surgical movement and, ultimately, facial changes, the orthodontist must carefully assess patients with musculoskeletal deformities before orthodontic treatment is begun. Accurate preoperative orthodontic and surgical planning that considers the indicated surgical movement is necessary to ensure not only good functional results but also an optimal esthetic outcome.
As seen in the patient in Fig 1-1, the dentition has been compromised for skeletal vertical maxillary excess and mandibular anteroposterior deficiency. Function and questionable stability have been achieved; however, the esthetic result is poor. An acceptable result is achieved after surg...