Written in a unique and innovative style, this book presents pediatric surgery in an interactive clinical context. Each chapter is built upon a specific disease or group of diseases, beginning with a typical case, presented interactively, just as it would be in encountered in clinical practice. These are actual cases that have been encountered by the author and are likely to be managed on any pediatric surgical service. The discussion that follows presents the most relevant issues pertaining to the topic, drawing on the index case, as well as multiple other cases that depict the entire spectrum of the disease or anomaly. The carefully selected suggested readings emphasize sentinel papers, high-quality reviews, and the best and most recent evidence published on the subject. A large number of illustrations help bring the clinical concepts to light. A number of high-quality videos provide a dynamic atlas of common procedures. The book is useful to the entire range of pediatric surgical trainees and practitioners, from the medical student or resident rotating on pediatric surgery, to the fellow preparing for certification, to the seasoned surgeon looking for an update on a particular subject or preparing for recertification. A large number of other physicians will find this book very useful, including general surgeons who evaluate and treat childhood surgical diseases, paediatricians and pediatric hospitalists who co-manage patients with surgeons, and obstetricians, pathologists, and radiologists who work closely with pediatric surgeons.
Key Features
Provides a hands-on guide to the management of typical clinical scenarios for all pediatric surgery trainees and other professionals involved in the care of childhood surgical disease
Presents more than 300 cases, covering the whole spectrum of pediatric surgery, illustrated in full-color and with an accompanying e-book
Allows the reader to apply their knowledge to real-life situations and assess their level of expertise by the use of a case-based Q&A format
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Clinical Pediatric Surgery est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Clinical Pediatric Surgery par Sherif Emil en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Medical Theory, Practice & Reference. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Index Case: Infant with Scrotal Mass and Irritability
You are consulted by the emergency department on a 10-week-old baby boy brought in by his mother for a right scrotal swelling, irritability, and two episodes of vomiting after breastfeeding. The baby was born at 32 weeks of gestation and discharged at 37 weeks postconceptual age. He has been doing well at home for the last 6 weeks. He was seen by one of your partners last week and diagnosed with a right inguinal hernia. Review of your partner’s note reveals that the hernia was reduced in the clinic with little difficulty. He is scheduled for surgery next week.
The mother notes that the hernia appeared larger than usual today, and the baby has been irritable. She tried to push on the hernia but it seemed painful. He has also been crying almost continuously for the last 2 hours and has been difficult to console.
Q1: How will you decide if this hernia is now incarcerated?
By definition, an incarcerated hernia is one that is not reducible. However, prior to attempting reduction, some aspects of the history, physical examination, and potential imaging may point to an incarceration and possible strangulation. Any history of bilious emesis or bloody stools should be elicited. The vital signs and perfusion status of the baby should be assessed. The abdomen should be examined for distention and peritoneal signs. The scrotum should be examined for possible redness or discoloration. Laboratory tests, including a complete blood count and a capillary blood gas should be checked if there is suspicion of bowel compromise. An abdominal film should be performed if there is suspicion of bowel obstruction.
The baby has had two episodes of non-bilious emesis and no bloody stools. Exam shows a baby who weighs 3.2 kg, with a heart rate of 180 beats per minute, but the other vital signs are normal. He is well perfused. The abdomen is soft and non-distended. The right scrotum is enlarged as shown in Figure 18.1. It is not discolored. However, it is tense and the baby starts to cry as soon as you touch it. Complete blood count shows a mildly elevated white blood cell count. The blood gas reveals no acidosis and a normal lactate level.
Figure 18.1 Right inguinal hernia
Q2: Should you try to reduce this hernia?
Yes. There are no signs of strangulation on the assessment. An attempt at reduction is warranted.
Q3: The emergency room resident offers to provide deep sedation for the reduction. Is this advisable?
In older children, deep sedation can be of significant help in a difficult reduction and should be well tolerated. However, in a baby with a history of significant prematurity, sedation may be quite risky and may lead to apnea and emergent intubation. Most physicians therefore will not use deep sedation when trying to reduce an inguinal hernia in an ex-premature baby.
You provide the baby with a sucrose-soaked pacifier and put him in Trendelenburg position in a dimly lit room for about 15 minutes before attempting reduction. The parents are by the bedside, and he is calm when you approach him.
Q4: How will you actually attempt to reduce this hernia?
Reduction of an incarcerated hernia is more likely to be successful if there is patience and persistence. The surgeon should not “fight” with the hernia. Significant pressure on the hernia is likely to elicit pain, leading to more straining by the baby and assured failure. One hand should push the inguinal component gently toward the scrotum, preventing the hernia from moving above the superficial inguinal ring. The other hand should support the scrotum and provide gentle continuous pressure toward the inguinal canal. This should be continued for 10–15 minutes before attempted reduction is abandoned. At no time should the surgeon attempt to “squeeze” the hernia into the abdomen. The reduction is successful if the hernia contents return to the abdomen and the baby experiences relief.
Despite trying for 20 minutes, you are unable to reduce the hernia or make sufficient progress. The baby starts to cry again and looks quite irritable. You book the baby for an emergency operation.
Q5: What potential interventions and complications should you discuss with the parents as part of obtaining consent?
Urgent repair of an incarcerated hernia is associated with higher complications versus elective inguinal hernia repair. There are several issues to discuss with the parents. The incarceration may have already compromised blood flow to the testicle, resulting in future decreased growth or atrophy of the testicle. If necrotic bowel is found, a bowel resection will be required with its attendant risks. There is a risk of injury to the vas deferens or testicular vessels, as well as a risk of recurrence. Finally, the potential to explore the contralateral side and repair a synchronous patent processus vaginalis should be discussed.
Q6: Will you perform an open or laparoscopic surgical procedure?
No studies have compared laparoscopic and open inguinal hernia repairs specifically in the setting of incarceration. Both procedures are appropriate. Open repair of an inguinal hernia in an ex-premature baby is frequently a challenging procedure and is even more difficult in the setting of incarceration. Laparoscopy does offer several advantages in this setting. Reduction is often facilitated by the pneumoperitoneum dilating the internal ring. The bowel can be directly examined for any signs of irreversible ischemia and exteriorized through a small extension of the umbilical incision for resection, if needed. The retroperitoneal edema at the internal ring often facilitates the laparoscopic repair by creating more space between the peritoneum and the vas deferens and testicular vessels. The contralateral deep ring can be assessed and repaired through the same incisions, if required. Finally, in some cases with a widely patent processus vaginalis, the testicle can be seen and assessed for ischemia.
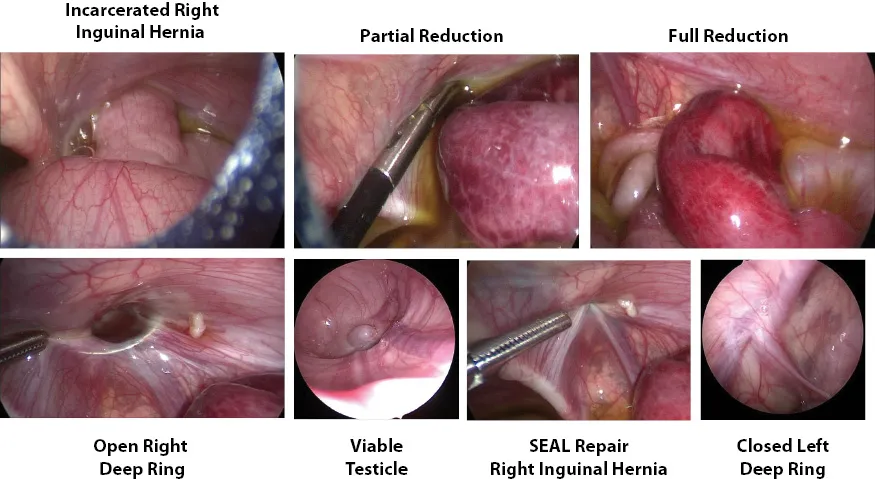
The surgical findings are shown in Figure 18.2. Severely congested, dilated small bowel is easily reduced. The bowel is not necrotic and starts to show evidence of recovery during the course of the case. The contralateral ring is closed. The right testicle is slightly dusky but viable. A subcutaneous endoscopic assisted ligation (SEAL) repair of the right inguinal hernia is performed.
Figure 18.2 Surgical findings
Q7: How should this baby be treated during the postoperative period?
This is an ex-premature baby who is currently 42 weeks postconceptual age. Admission for 24 hours of cardiorespiratory monitoring is indicated. Analgesia can be given in the form of around-the-clock acetaminophen, but no narcotics should be used. Breastfeeding may be started in the recovery room. The baby may be discharged if there are no apneas or bradycardias during the observation period.
The baby’s recovery is uneventful and he is discharged after 24 hours.
Q8: What are the specific conditions you will screen for at the baby’s follow-up?
The main potential complications of the presentation and operation are hernia recurrence and testicular atrophy or asymmetric testicular growth. Residual hydroceles after laparoscopic hernia repair in small infants may occur but are usually less impressive than those seen after open repairs. They typically resolve spontaneously.
The baby is first seen 1 month after discharge. There are no signs of recurrence. The right testicle is thickened compared to the left, and a small right hydrocele is seen. Follow-ups at 6 months show normal exams with no signs of recurrence and symmetric testicles.
Discussion
Abdominal wall hernias, specifically inguinal and umbilical hernias are the “bread and butter” of pediatric surgery, the most common elective cases in many pediatric surgical practices. Other less-frequent abdominal wall hernias and defects assessed and managed by pediatric surgeons include epigastric hernias, supra-umbilical hernias, abdominal wall eventrations, lumbar hernias, Spigelian hernias, diastasis recti, and prune belly syndrome.