
eBook - ePub
Respiratory Diseases of the Horse
A Problem-Oriented Approach to Diagnosis and Management
Laurent Couetil, Jan F Hawkins
This is a test
Partager le livre
- 256 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Respiratory Diseases of the Horse
A Problem-Oriented Approach to Diagnosis and Management
Laurent Couetil, Jan F Hawkins
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
The authors provide a problem-oriented approach to the assessment and management of respiratory illness in horses. The book deals first with the anatomy, function and clinical examination of the respiratory system, followed by discussion of diagnostic tests and procedures. The clinical section is focused around the cardinal presenting manifestation
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Respiratory Diseases of the Horse est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Respiratory Diseases of the Horse par Laurent Couetil, Jan F Hawkins en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicina et Medicina veterinaria. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
CHAPTER 1
ANATOMY OF THE EQUINE RESPIRATORY TRACT
INTRODUCTION
The anatomy of the respiratory tract greatly influences its function (1). Additional factors, such as exercise, will result in further adaptation of the respiratory tract anatomy by increasing contraction of the accessory respiratory muscles to accommodate the increase in ventilation or exercise-induced hyperpnea. From a functional standpoint, it is helpful to separate the respiratory tract into the extrathoracic airways and the intrathoracic airways, with the former extending from the nose to the extrathoracic portion of the trachea.
EXTRATHORACIC AIRWAYS
Overview
The main role of the airways is to act as a conduit for air flow between the nasal opening and the gas-exchanging areas of the lung. To accommodate convection of air, the extrathoracic airways, and in particular the nasal passages, modify the air by adjusting its temperature nearer to normal body temperature, increasing the relative humidity closer to full saturation, and by filtering larger particles. The total cross-sectional area of the proximal respiratory tract is minimal compared with the vast surface area of the distal airways (bronchioles) and alveolar spaces. Any disease resulting in a decrease in airway patency will impair airflow and, ultimately, pulmonary function; however, a decrease in airway diameter will have maximum impact if located along the proximal airways, since all air travels through this bottleneck. In contrast, diseases involving the distal airways in the lung have to be severe and extensive to cause flow limitation. At rest, horses use only a small portion of their vital respiratory capacity (approximately 10%), so diseases resulting in airway obstruction have to be severe in order to impair pulmonary function. During strenuous exercise, horses utilize 100% of their respiratory capacity and mild airway obstruction that would not normally affect pulmonary function at rest may greatly interfere with gas exchanges during exercise.
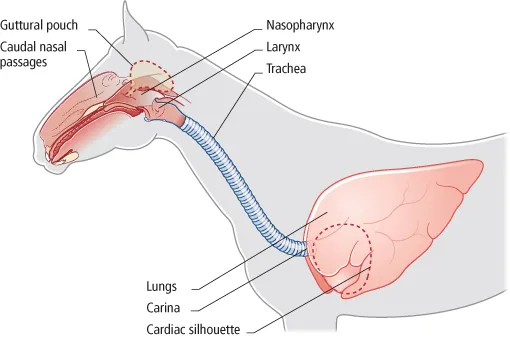
1 Anatomy of the equine respiratory tract, with anatomic regions corresponding to endoscopic views in the following figures: caudal nasal passages (6); guttural pouch (15); nasopharynx (19); larynx (20); trachea (37); carina (41).
Assessment of diseases of the extrathoracic airways requires a full understanding of the unique anatomic features of the equine proximal respiratory tract (PRT). Knowledge of the gross and endoscopic anatomy of the PRT is crucial to arriving at a working diagnosis in a horse with clinical signs of respiratory noise and exercise intolerance. The normal anatomy of the structures (nares and rostral nasal passages, nasal septum, conchae and paranasal sinuses, guttural pouches (GPs), nasopharynx, hard and soft palate, epiglottis, larynx, and cervical portion of the trachea) that make up the equine PRT are described below.
Nares and rostral nasal passages
Airflow from the left and right nares should be equal and easily palpable or visualized by movement of soft cotton or condensation on a mirror (2).
The nares consist of the nasal opening, alar folds, nasal diverticulum, and the rostral aspect of the nasal septum (3).
2 Subjective evaluation of palpable airflow from each nasal passage. Clinical assessment of airflow can be enhanced by the use of a rebreathing bag.

3 Gross postmortem photograph illustrating the cut edge of the nasal diverticulum (yellow arrows), alar fold (black arrow), and rostral nasal septum (red arrow). (D) dorsal; (Ro) rostral.

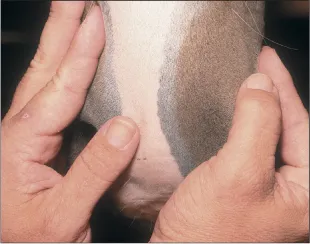
4 Manual palpation of the rostral nasal septum.
The false nostrils should be capable of full and symmetrical opening. The alar fold should be thin, pliable, and not edematous. The nasal diverticulum is located dorsal to the alar fold. The rostral aspect of the nasal septum is palpated manually with the index fingers (4). The normal rostral nasal septum is bilaterally symmetrical and the mucosa should be smooth and have no appreciable pitting edema.
Nasal septum
The equine nasal septum consists predominantly of fibrocartilage (5). The ventral aspect of the nasal septum is attached to the vomer bone. A normal nasal septum should be straight and not deviated towards either nasal passage. It is covered by nasal mucosa.
The nasal cavities are lined with a richly vascularized mucosa to allow warming and humidification of inhaled air. Vasomotor tone is under the control of the autonomic nervous system, with excitation of sympathetic and parasympathetic nerves leading to nasal vasoconstriction and vasodilation, respectively. Exercise is associated with sympathetic excitation and increased nasal volume. Despite these mechanisms, which are designed to increase airway patency during exercise, the nasal passages still represent one of the bottleneck regions of the equine respiratory tract.
Conchae and paranasal sinuses
The horse has seven paranasal sinuses on each side of the skull. These are the dorsal, middle, and ventral conchal sinuses, the rostral and caudal maxillary sinuses, the frontal sinus, and the sphenopalatine sinus. The conchae and sinuses communicate through multiple natural openings. The dorsal and middle conchal, sphenopalatine, and frontal sinuses communicate with the caudal maxillary sinus. The ventral conchal sinus communicates with the rostral maxillary sinus. The nasomaxillary opening is the communication between the nasal passage and the maxillary sinus (6). It is located in the middle meatus in the area of the ethmoid turbinate and it can be visualized with an endoscope.
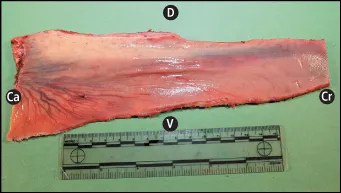
5 Gross postmortem appearance of a normal nasal septum. Note the prominent vascular pattern on the caudal and ventral aspect of the septum. (Ca) caudal; (Cr) cranial; (D) dorsal; (V) ventral.
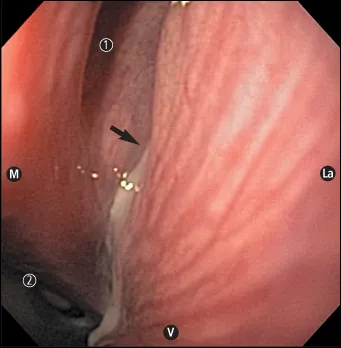
6 Endoscopic view of the left nasomaxillary opening (arrow) with purulent exudate exiting the maxillary sinus. (1) ethmoid turbinates; (2) nasopharynx; (La) lateral; (M) medial; (V) ventral.
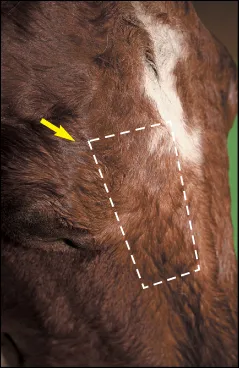
7 Gross postmortem appearance of the surgical limits of the frontal sinus (dotted line). Arrow, supraorbital foramen.
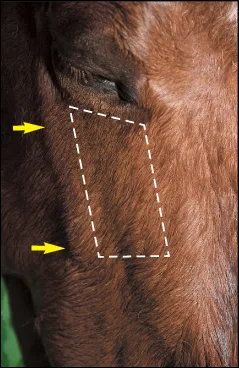
8 Gross postmortem photograph illustrating the boundaries of the maxillary sinus (dotted line). Arrow, facial crest.
Along with an understanding of the natural openings between the sinuses, the surgical limits of the frontal and maxillary sinuses should also be known. The surgical limits of the frontal sinus are: medially, the midline of the forehead; caudally, a line joining the right and left supraorbital foramina; rostrally, a line approximately 8–10 cm rostral, or a line perpendicular to the facial crest, half-way between the medial canthus and the infraorbital foramen; and laterally, a line drawn from the medial canthus of the eye to the nasoincisive notch (7).
The surgical limits of the maxillary sinus are: dorsally, a line from the medial canthus of the eye to the infraorbital foramen; caudally, a line from the medial canthus to the facial crest; rostrally, a line from the infraorbital foramen to the facial crest; and ventrally, the facial crest (8).
Other important anatomic features of the frontal and maxillary sinuses include the following:
• The rostral limit of the frontal sinus is 2–3 cm from where the nasal bones diverge and the calvarium is close to the caudal limit of the sinus (9). Therefore, it is very important not to go beyond the supraorbital foraminae when surgically opening the frontal sinus.
• At the rostral end of the frontal sinus there is a large medial and ventral communication with the dorsal conchal sinus (10). At this point the common area between the two is called the conchofrontal sinus. The ethmoidal labyrinth is located on the floor of th...