
eBook - ePub
Rheumatology
A Color Handbook
Ted Mikuls, Amy Cannella, Gerald Moore, James O'Dell, Alan Erikson, Geoffrey Thiele
This is a test
Partager le livre
- 224 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Rheumatology
A Color Handbook
Ted Mikuls, Amy Cannella, Gerald Moore, James O'Dell, Alan Erikson, Geoffrey Thiele
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
This book provides the reader with a complete and concise introduction to rheumatic illness. While rheumatic disease often manifests itself in conditions affecting the musculoskeletal system, the authors stress that a comprehensive multidisciplinary approach is needed for diagnosis, to aid understanding of rheumatic disease with multisystem involve
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Rheumatology est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Rheumatology par Ted Mikuls, Amy Cannella, Gerald Moore, James O'Dell, Alan Erikson, Geoffrey Thiele en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Médecine et Théorie, pratique et référence de la médecine. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
CHAPTER 1
Overview of Rheumatology and Rheumatic Conditions
• Introduction
• Synopsis of immunology in rheumatic disease
• Assessment of the patient with a suspected rheumatic condition
• Pregnancy in rheumatic diseases
• Pharmacological treatment of rheumatic disease
• Nonpharmacological treatment of rheumatic disease

Introduction
RHEUMATOLOGY AND RHEUMATIC CONDITIONS – OVERVIEW
Rheumatology is an internal medicine and pediatric subspecialty focused on the diagnosis and management of diseases affecting primarily the joints and surrounding soft tissues. Rheumatic conditions are composed of arthritis and its allied connective tissue diseases. The term ‘arthritis’ is derived from the Greek ‘arthro’ (meaning joint) and ‘-itis’ (meaning inflammation). There are currently more than 100 discrete forms of arthritis recognized, the most common being osteoarthritis (OA). Arthritis is often categorized by its distribution (monoarticular vs. polyarticular); its association with detectable autoantibody (seropositive vs. seronegative); or the degree of underlying inflammation involved (inflammatory vs. noninflammatory. (The latter is a misnomer since nearly all forms of arthritis are characterized by at least low-grade inflammation).
By the very nature of the multisystem diseases encountered in rheumatology, this is a field with multidisciplinary facets that include nearly all other subspecialties in medicine in addition to other major fields of study (genetics, psychiatry, surgery, dermatology, neurology, and so on). A review of the diagnostic criteria for systemic lupus erythematosus (SLE), a condition encountered in the rheumatology clinic on a near daily basis, illustrates the cross-disciplinary nature of this subspecialty. Major advances in immunology and an increased understanding of disease pathogenesis show that many rheumatic conditions can be characterized as ‘autoimmune diseases’ (autoimmunity can be simply defined as immune responses against ‘self’). SLE, for example, is characterized by the presence of antinuclear antibody (ANA), while recent advances have shown that anticitrullinated protein antibody (anti-CCP antibody) are nearly exclusive to patients with rheumatoid arthritis (RA).
IMPACT OF RHEUMATIC CONDITIONS
Arthritis and its allied health conditions are highly prevalent with musculoskeletal complaints accounting for one in five to one in 10 of all primary care visits. Prevalence rates for different forms of arthritis and allied conditions are summarized in Table 1. The US Centers for Disease Control and Prevention (CDC) estimates that nearly 20% of American adults suffer from physician-diagnosed arthritis. Similar prevalence rates of arthritis have been reported from other developed countries. With an aging population, the burden posed by arthritis and its allied health conditions is expected to grow, with more than 67 million adults expected to have arthritis in the next 20 years. Arthritis and related conditions are the leading cause of disability in many countries worldwide (1). Arthritis and rheumatism, along with back problems, account for approximately one in every three cases of disability. Not surprisingly, the direct and indirect costs associated with the care of rheumatic disease are enormous. In 1997, it was estimated that arthritis and its allied conditions were associated with total societal costs of US $116 billion – 1.4% of the gross domestic product. With the availability of newer (and more expensive) therapies, these costs have likely grown. In addition to associations with work-related disability and rising healthcare costs, many rheumatic diseases (e.g. RA, SLE, scleroderma [SSc]) are associated with increased morbidity and accelerated mortality.
Table 1 Estimated prevalence of select forms of arthritis and allied conditions among adults in the US*

MAJOR TREATMENT ADVANCES
Recent improvements in our understanding of immunology and disease pathogenesis have led to seminal advances in the management of the rheumatic diseases. In the last decade alone, there have been at least seven biologic, disease-modifying, antirheumatic drugs (DMARDs) approved for the treatment of RA, with many of these agents also approved for the treatment of juvenile idiopathic arthritis (JIA), seronegative spondyloarthropathy, and inflammatory bowel disease. Recent advances have yielded important alternatives for the treatment of end-organ involvement in SLE and, for the first time in more than 40 years, new treatment options are available for patients with chronic gout.
With the availability of a rapidly expanding treatment armamentarium in rheumatology, the importance of early diagnosis and intervention becomes even more evident. In this textbook, we provide an introduction to the rheumatic conditions, including concise reviews of arthritis and its many allied health conditions. The aim of this textbook is to familiarize general practitioners, medicine trainees, and other ancillary healthcare personnel involved in the care of patients with rheumatic disease with the major tenets of disease epidemiology, pathogenesis, diagnosis, and management in rheumatology.
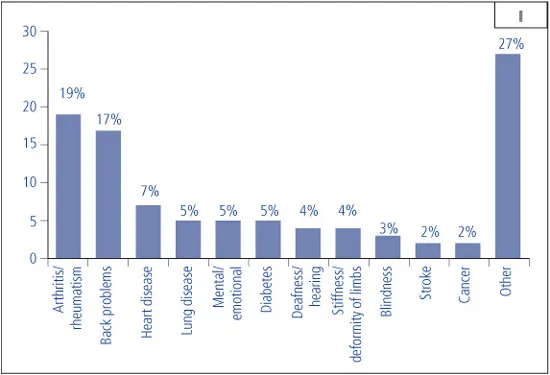
1 Primary causes of disability among adults in the US, 2005 (Source: US Census Bureau, Survey of Income and Program Participation).
Synopsis of immunology in rheumatic disease
INTRODUCTION
The immune response is composed of antigen nonspecific and specific elements that can initiate the recruitment of cells and secretion of factors that induce inflammation. This process is efficient at removing pathogenic organisms (i.e. viruses, fungi, bacteria), but immune-mediated tissue injury can occur as part of this response. Moreover, dysregulation of the immune/inflammatory response may then lead to the steps resulting in autoimmune diseases. Add to this the hormonal and environmental factors that influence immune responses, as well as the molecular basis of autoimmune disease, and the pathogenesis of rheumatic diseases is extraordinarily complex. This section provides an outline of the important features of the immune system, including some of its most critical cells and molecules, and the principles that relate to the pathogenesis of immune-mediated diseases.
INNATE IMMUNE SYSTEM
Definition
• No specificity to an antigen.
• No memory for an antigen.
• 80–90% of all immune responses occur through this branch of the immune system.
Mechanisms of action
Exterior defenses:
• Physical defenses:
• Skin – epithelial cells.
• Cilia – on mucosal cells beat outward.
• Mucus – has a washing effect.
• Stomach acid – pH 1.5–2.0.
• Tears – washing effect.
• Biochemical defenses:
• Enzymes – degrade proteins and nucleic acids (i.e. lysozyme in tears).
• Sebaceous glands – release oils that are bacteriostatic or bactericidal.
• Commensal organisms – ‘normal flora’ in the gut, vaginal area, other mucosal sites.
Cells:
• Phagocytes. While many cell types have phagocytic capabilities, the two major cells of the immune system that perform this function are:
• Mononuclear phagocytes
1 Macrophages – general term related to these cells throughout the body.
2 Monocytes – found in the blood.
3 Histiocytes – specific for a tissue.
i Kupffer cells = liver.
ii Microglial cells = brain.
iii Synovial A cells = joints.
iv Mesangial cells = kidney.
• Neutrophils
1 Polymorphonuclear neutrophils.
2 Predominant cells making up the white blood cell (WBC) count (~70% WBCs).
3 Have granules inside the cell that contain enzymes.
• Recognition of ‘foreign agents’.
• Pathogen-associated molecular patterns (PAMPs) includes: sugars, proteins, lipids, nucleic acids or their combinations.
• Pattern recognition receptors (PRRs) are the toll-like receptors or scavenger receptors.
• PAMPs on a pathogen are recognized by PRRs on phagocytes that result in:
1 Elevated microbial activity; peroxide, superoxide, degradative enzymes, and so on.
2 Increased expression of adhesion molecules and co-stimulatory molecules.
3 Phagocytosis.
i The engulfment and destruction of the pathogen.
ii Opsonization.
a) Some molecules (acute phase proteins, i.e. C-reactive protein [CRP], serum amyloid A [SAA], mannose-binding lectin, and so on) attach to the surface of the pathogen (opsonins) and bind to receptors on the phagocytes.
b) Results in an enhanced phagocytosis.
ADAPTIVE IMMUNE SYSTEM
Definition
The adaptive immune system is:
• Specific for an antigen.
• T cell = T cell receptor (TCR, Table 2)
• B cell = surface immunoglobulin (sIg) receptor (antibody that is never secreted, 2)
• Capable of forming memory for an antigen.
• First exposure primes the system with little or no response.
• Second exposure results in increased memory and amplification of the immune system.
Table 2 Definitions of common immunologic terms
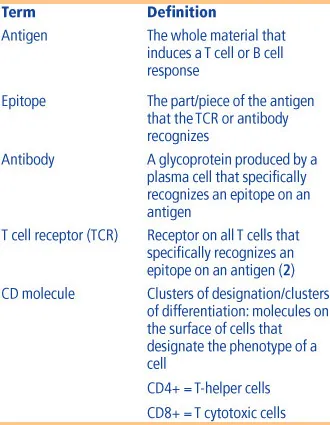
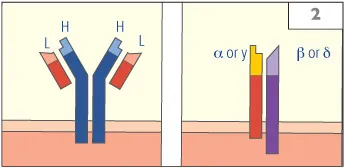
2 Antigen specificity in the adaptive immune system occurs first at the B cell and T cell levels. The specificity for B cells is conferred through the B cell receptor also known as the surface immunoglobulin (sIg) receptor. This immunoglobulin is surface bound and is never secreted. It is comprised of two identical heavy chains (H) and two identical light chains (L) that have an antigen binding site at the tip where these two proteins meet. When a B cell is activated through binding of antigen to this binding site on a sIg, the B cell under the right conditions will differentiate into a plasma cell and secrete antibody of the same specificity as the sIg.
The T cell receptor has an antigen binding site at the tip of one alpha (α) and one beta (β) chain. This type of T cell recepto...